 |
| Few US citizens get all the nutrients they need from their diets. |
The bad news first: The study found sign. deficiency rates for all the investigated nutrients: vitamins A, B6, B12, C, D, E, folate and iron. The good news: It's easy and - with the exception of iron and folate 100% unproblematic to supplement your diet.
Looking for more ways to improve your diet? Increase your potassium (K) intake!

Potassium vs. Diet-Inducded Insulin Resis.

In the Lime Light: The Ill Effects of Low K Intakes

Bad News: Most Americans are Sign. K Deficient

Lean, Healthy ... Correlates of High Hair Potassium

Eating a High Protein Diet? Better Watch K!

Potassium Bicarbonate = Anabolic!?
 |
| Table 1: Proportion of the population with usual intakes below the EAR (estimated average requirement), the RDA (recommended dietary allowance) and excessive intake according to TUL (total upper limit | Bird 2017) |
- significantly higher deficiency risks in women (37%), non-Hispanic blacks (55%), individuals from low-income households (40%), or without a high school diploma (42%);
- significantly higher deficiency risks in underweight (42%) or obese individuals (39%);
- that women aged 19–50 years (41%), and pregnant or breastfeeding women (47%) are at particular risk of nutrient deficiencies;
- that dietary supplement non-users had the highest risk of any deficiency (40%), compared to users of full-spectrum multivitamin-multimineral supplements (14%) and other dietary supplement users (28%)
The symptoms that can arise from not getting enough of these nutrients (you don't have to get 100% every day, though) range from
- impaired immunity, growth and night blindness from vitamin A deficiency, over
- impaired wound healing and bleeding from vitamin C deficiency,
- anemia from iron deficiency, and
- rickets and osteomalacia from vitamin D deficiency, to
- megaloblastic anemia with low folate intakes,
- microcytic anemia with B6 deficiencies, and
- pernicious anemia and neurological damage due to impaired myelination with low B12.
"For example, erythropoiesis requires not only iron, but also folate, vitamin B12, and vitamin A, and dietary vitamin C can improve the absorption of non-heme iron. Sub-clinical deficiency symptoms for many vitamins and minerals are non-specific, and may include fatigue, irritability, aches and pains, decreased immune function, and heart palpitations" (Bird 2017).
Previous reports estimated the deficiency prevalence for each of the vitamins B6, C, and D, and the mineral iron, between 5–10% (similarly, previous studies underestimated the risk of missing out on not just one but two nutrients, i.e. 5.7% vs. 23%).
What kind of data are we talking about? Food questionnaires? Yes, we are talking about questionnaires (two 24h recalls, to be specific), but the scientists also used data from blood draws that were conducted as part of the NHANES cycles.
If you take another look at Table 1 the study at hand found significantly higher prevalences of nutrient deficiency. Racial and social disparities have been observed before, but the prevalence rates in risk groups such as pregnant and breastfeeding women, low-income households, or according to educational status, body mass index (BMI), or measures of dietary intake have not been investigated previously.
 |
| Figure 1: Risk of biochemical vitamin deficiency or anemia, by DS use and dietary vitamin/mineral inadequacy/insufficiency (Bird 2017). |
All that is bad news, but the fact that only a small number of subjects ended up above the Tolerable Upper Limit (TUL) was low - 1.1%, 0.68%, and 0.31% of the population had excessive intakes of iron, folate, and retinol, respectively - is unquestionably good news. After all, all three of them have potentially health-threatening side effects, most prominently, probably the birth defects (> 8,000 IU / day), risk of osteoporosis, hair loss, bone pain, elevated blood sugar, liver damage, and liver damage (> 25,000 IU / day) for retinol (vitamin A).
What about athletes and gymrats
The data from studies in athletes tend to show generally reduced risks of nutrient deficiency because (a) athletes tend to eat more, (b) athletes tend to eat more healthy, and (c) athletes tend to take more supplements. For their immune-competence, an adequate intake of iron, vitamins A, E, B6 and B12 is particularly important for athletes (Gleeson 2001).
Interestingly enough, the IOC only recently warned about general energy deficiencies in athletes. In fact, next to sports of which you'd already expect that athletes purposefully consume less than optimal amounts of energy, you can see in Table 2, that other sports, like Tour de France cycling, simply burn so much energy that the athletes cannot keep up (Meyer 2016). For many athletes, this lack of energy intake translates into a lack of micronutrients - with calcium and vitamin D deficits being both prevalent and risky; risky because they significantly increase the risk of stress fractures.
Isn't is obvious that everyone should take a multi? Not really.... While this is what the industry wants to make you believe, the actual scientific evidence that taking a multi-nutrient supplement is good for you is... well let's say "inconclusive". There's, for example, the claim that B-vitamins will combat the cognitive decline with age - which makes absolute sense, theoretically, has been observed in some trials (e.g. Douaud 2013), but is not supported by the majority of RCTs and epidemiological studies (Raman 2007; Kang 2008; Wald 2010). In contrast to popular claims, B-vitamin supplementation doesn't lower cardiovascular disease, cancer, and cause-specific mortality, either (Clarke 2010).
Similarly disappointing results have been reported for multivitamin supplements by Grodstein et al. (2013) - with respect to dementia. Likewise a null-result was reported by Macpherson et al. (2013) who didn't find sign. effects on all-cause mortality in their meta-analysis. Multis don't seem to reduce the infection risk in the elderly (El-Kadiki 2005). They don't reduce the risk of progression atherosclerosis (Bleys 2006) or protect you from CVD (Myung 2013). They don't protect you from prostate or breast cancer (Stratton 2011; Chan 2011) and/or general cancer mortality (Park 2011). And the list can be extended (e.g. Song 2011; Sesso 2012...).
For specific vitamins, like vitamin E, the evidence is even downright disconcerting. Next to evidence suggesting that it's only useless (Vivekananthan 2003), there are also studies showing increased mortality with high(er) doses (>400IU per day | Miller 2005) and an increased risk of stroke (Schürks 2010), which is the exact opposite of what you see with veggies and fruit (He 2006). Just as usual, there's yet also evidence to the contrary. Ye & Song report a reduced risk of coronary heart disease in their meta-analysis of cohort studies (Ye 2008) - and guess what: they analyzed data from studies that used the often bashed vitamins C+E + beta carotene.
So what? Well, if you asked me: I still think it's not necessary. A low (RDA) dosed multi is yet probably not going to kill you (or what frightens some readers even more "impair your gains" - that takes much higher doses of vitamin C + E than the RDA).The #1 deficiency in athletes is yet one that you will find in the general population, as well. Iron deficiencies (Zourdos 2015)... and that often in the presence of normal hemoglobin values:
The likewise prevalent deficiencies in magnesium and zinc can have similar, albeit less far-reaching ill effects on athletes' performance; just as other less prevalent nutrient deficiencies of Dutch athletes, you can delineate from the data in Table 3.
Bottom line: Better safe than sorry? When we're talking about classic "multis" or FSMRs as they were called in the study at hand, the strategy the scientists describe as "nutritional insurance to cover unintended gaps in dietary intakes" probably isn't the worst one (cf. Bailey 2013).
This is especially true, because many classic deficiency nutrients were not even included in the analysis: vitamin D, of which 14-18% of all US citizens have way too little (full deficiency w/ 25(OH)D <40 nmol/L) in their blood (Schleicher 2016), zinc deficiency (a global problem esp. for women | Hess 2017), or magnesium deficiency which plagues every third American and of which 62% get only insufficient amounts (Deng 2013).
Needless to say: Logging your food intake over 1-2 weeks and calculating potential deficiencies to then buy exactly the supplements you really need would be the better choice. Even better probably than many of the expensive tests, the accuracy or relevance (e.g. serum magnesium = not representative of your real magnesium status) of which is vastly overstated by their providers.
Also, if you want to know more, catch up w/ previously discussed nutrient deficiency articles on choline, various nutrients, potassium | Or tell me what you think in a comment on Facebook!References:
What about athletes and gymrats
The data from studies in athletes tend to show generally reduced risks of nutrient deficiency because (a) athletes tend to eat more, (b) athletes tend to eat more healthy, and (c) athletes tend to take more supplements. For their immune-competence, an adequate intake of iron, vitamins A, E, B6 and B12 is particularly important for athletes (Gleeson 2001).
Are "natural vitamins" better than "artificial" ones? For many vitamins, the "natural" version isn't better than "artificial" one. For others there's good evidence (discussed here) in favor of "natural vitamins"; and, even more importantly, if you get the vitamins from whole foods you usually get all necessary co-factors you will be missing w/ most of the dietary supplements (natural or artificial).
It should be emphasized, though, that "acute or short-term marginal deficiencies, identified by blood biochemical measures of vitamin B status, [have] no impacts on performance measures" (Lukaski 2004). Particularly folate and B12 are still deficiency nutrients - especially in endurance athletes who will often suffer from anemia as a consequence of not getting enough of these important B-vitamins. "Evidence of vitamin A and E deficiencies in athletic individuals is lacking apparently because body storage is appreciable" (Lukaski 2004).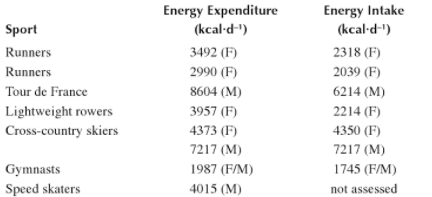 |
| Table 2: Energy expenditure in various sports - measured by doubly-labeled water compared to data from dietary recall, (M) male subjects, (f) female subjects (from Meyer 2016) |
 |
| Cumulative meta-analysis of the effect of vitamin B supplementation on the risk of cancer incidence (A), death due to cancer (B), and total mortality (C | Zhang 2016). |
Similarly disappointing results have been reported for multivitamin supplements by Grodstein et al. (2013) - with respect to dementia. Likewise a null-result was reported by Macpherson et al. (2013) who didn't find sign. effects on all-cause mortality in their meta-analysis. Multis don't seem to reduce the infection risk in the elderly (El-Kadiki 2005). They don't reduce the risk of progression atherosclerosis (Bleys 2006) or protect you from CVD (Myung 2013). They don't protect you from prostate or breast cancer (Stratton 2011; Chan 2011) and/or general cancer mortality (Park 2011). And the list can be extended (e.g. Song 2011; Sesso 2012...).
For specific vitamins, like vitamin E, the evidence is even downright disconcerting. Next to evidence suggesting that it's only useless (Vivekananthan 2003), there are also studies showing increased mortality with high(er) doses (>400IU per day | Miller 2005) and an increased risk of stroke (Schürks 2010), which is the exact opposite of what you see with veggies and fruit (He 2006). Just as usual, there's yet also evidence to the contrary. Ye & Song report a reduced risk of coronary heart disease in their meta-analysis of cohort studies (Ye 2008) - and guess what: they analyzed data from studies that used the often bashed vitamins C+E + beta carotene.
So what? Well, if you asked me: I still think it's not necessary. A low (RDA) dosed multi is yet probably not going to kill you (or what frightens some readers even more "impair your gains" - that takes much higher doses of vitamin C + E than the RDA).
"De Wijn et al. reported that 7% of male and 17.5% of female athletes studied had a transferrin saturation index be low 20% [you need to have both, a high transferrin saturation andenough serum iron], but very few were anaemic.
Figure 2: Treatment algorithm based on plasma ferritin and haemoglobin levels (C reactive protein is considered normal). Hb = haemoglobin (Chatard 1999).

Clement et al. (1977) studied elite Canadian endurance runners, and found that 29% of the men and 82% of the women had extremely low ferritin values (<25 µg/L), even though their blood haemoglobin and serum iron levels were normal" (Chatard 1999).Supplementation has been found to improve athletic performance significantly, even in marginal deficiency states (Schoene 1983) - even in the absence of anemia (Burden 2015). And while female athletes are for obvious reasons (menses) at highest risk of low iron, Peeling et al. argue quite convincingly that exercise induced inflammation, the release of cytokines, which increase the hormone hepcidin that in turn reduced impairs iron transport and absorption put athletes at particular risk of iron deficiencies (Peeling 2008).
 |
| Table 3: Adequacy of micronutrient intake (%) in men and women presented for users and non-users of nutritional supplements (Wardenaar 2017). Non-users of nutritional supplements (‘non-users’), users of dietary supplements (DS), users of sport nutrition products (SNP) and users of a combination of both (DS + SNP). |
 |
| The ill effects of cold-water immersion on muscle gains are just one out of dozens of examples, where things that should work - theoretically. |
This is especially true, because many classic deficiency nutrients were not even included in the analysis: vitamin D, of which 14-18% of all US citizens have way too little (full deficiency w/ 25(OH)D <40 nmol/L) in their blood (Schleicher 2016), zinc deficiency (a global problem esp. for women | Hess 2017), or magnesium deficiency which plagues every third American and of which 62% get only insufficient amounts (Deng 2013).
Needless to say: Logging your food intake over 1-2 weeks and calculating potential deficiencies to then buy exactly the supplements you really need would be the better choice. Even better probably than many of the expensive tests, the accuracy or relevance (e.g. serum magnesium = not representative of your real magnesium status) of which is vastly overstated by their providers.
Also, if you want to know more, catch up w/ previously discussed nutrient deficiency articles on choline, various nutrients, potassium | Or tell me what you think in a comment on Facebook!
- Bailey, Regan L., et al. "Why US adults use dietary supplements." JAMA internal medicine 173.5 (2013): 355-361.
- Bird, Julia K., et al. "Risk of Deficiency in Multiple Concurrent Micronutrients in Children and Adults in the United States." Nutrients 9.7 (2017): 655.
- Bleys, Joachim, et al. "Vitamin-mineral supplementation and the progression of atherosclerosis: a meta-analysis of randomized controlled trials." The American journal of clinical nutrition 84.4 (2006): 880-887.
- Burden, Richard J., et al. "Is iron treatment beneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? A systematic review and meta-analysis." Br J Sports Med 49.21 (2015): 1389-1397.
- Chan, Agnes LF, Henry WC Leung, and Shiao-Fung Wang. "Multivitamin supplement use and risk of breast cancer: a meta-analysis." Annals of Pharmacotherapy 45.4 (2011): 476-484.
- Chatard, Jean-Claude, et al. "Anaemia and iron deficiency in athletes." Sports Med 27.4 (1999): 229-240.
- Clement, D. B., R. C. Asmundson, and C. W. Medhurst. "Hemoglobin values: comparative survey of the 1976 Canadian Olympic team." Canadian Medical Association Journal 117.6 (1977): 614.
- Deng, Xinqing, et al. "Magnesium, vitamin D status and mortality: results from US National Health and Nutrition Examination Survey (NHANES) 2001 to 2006 and NHANES III." BMC medicine 11.1 (2013): 187.
- De Wijn, J. F., et al. "Hemoglobin, packed cell volume, serum iron and iron binding capacity of selected athletes during training." Annals of Nutrition and Metabolism 13.3-4 (1971): 129-139.
- El-Kadiki, Alia, and Alexander J. Sutton. "Role of multivitamins and mineral supplements in preventing infections in elderly people: systematic review and meta-analysis of randomised controlled trials." Bmj 330.7496 (2005): 871.
- Fortmann, Stephen P., et al. "Vitamin and mineral supplements in the primary prevention of cardiovascular disease and cancer: an updated systematic evidence review for the US Preventive Services Task Force." Annals of internal medicine 159.12 (2013): 824-834.
- Gleeson, Michael, Graeme I. Lancaster, and Nicolette C. Bishop. "Nutritional strategies to minimise exercise-induced immunosuppression in athletes." Canadian journal of applied physiology 26.S1 (2001): S23-S35.
- Grodstein, Francine, et al. "Long-term multivitamin supplementation and cognitive function in mena randomized trial." Annals of internal medicine 159.12 (2013): 806-814.
- Guallar, Eliseo, et al. "Enough is enough: stop wasting money on vitamin and mineral supplements." Annals of internal medicine 159.12 (2013): 850-851.
- He, Feng J., Caryl A. Nowson, and Graham A. MacGregor. "Fruit and vegetable consumption and stroke: meta-analysis of cohort studies." The Lancet 367.9507 (2006): 320-326.
- Hess, Sonja Y. "National risk of zinc deficiency as estimated by national surveys." Food and nutrition bulletin 38.1 (2017): 3-17.
- Kang, Jae Hee, et al. "A trial of B vitamins and cognitive function among women at high risk of cardiovascular disease." The American journal of clinical nutrition 88.6 (2008): 1602-1610.
- Meyer, Nanna L., and Melinda M. Manore. "2 Evaluation of Nutrient Adequacy of Athletes’ Diets." Nutritional Assessment of Athletes (2016): 51.
- Myung, Seung-Kwon, et al. "Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: systematic review and meta-analysis of randomised controlled trials." Bmj 346 (2013): f10.
- Lukaski, Henry C. "Vitamin and mineral status: effects on physical performance." Nutrition 20.7 (2004): 632-644.
- Park, Song-Yi, et al. "Multivitamin use and the risk of mortality and cancer incidence: the multiethnic cohort study." American journal of epidemiology 173.8 (2011): 906-914.
- Peeling, Peter, et al. "Athletic induced iron deficiency: new insights into the role of inflammation, cytokines and hormones." European journal of applied physiology 103.4 (2008): 381.
- Raman, Gowri, et al. "Heterogeneity and lack of good quality studies limit association between folate, vitamins B-6 and B-12, and cognitive function." The Journal of nutrition 137.7 (2007): 1789-1794.
- Schleicher, Rosemary L., et al. "The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases." The American journal of clinical nutrition 104.2 (2016): 454-461.
- Sesso, Howard D., et al. "Multivitamins in the prevention of cardiovascular disease in men: the Physicians' Health Study II randomized controlled trial." Jama 308.17 (2012): 1751-1760.
- Schoene, Robert B., et al. "Iron repletion decreases maximal exercise lactate concentrations in female athletes with minimal iron-deficiency anemia." The Journal of laboratory and clinical medicine 102.2 (1983): 298-305.
- Song, Yiqing, et al. "Multivitamins, individual vitamin and mineral supplements, and risk of diabetes among older US adults." Diabetes care 34.1 (2011): 108-114.
- Stratton, Julie, and Marshall Godwin. "The effect of supplemental vitamins and minerals on the development of prostate cancer: a systematic review and meta-analysis." Family practice 28.3 (2011): 243-252.
- Wald, David S., Anuradhani Kasturiratne, and Mark Simmonds. "Effect of folic acid, with or without other B vitamins, on cognitive decline: meta-analysis of randomized trials." The American journal of medicine 123.6 (2010): 522-527.
- Wardenaar, Floris, et al. "Micronutrient Intakes in 553 Dutch Elite and Sub-Elite Athletes: Prevalence of Low and High Intakes in Users and Non-Users of Nutritional Supplements." Nutrients 9.2 (2017): 142.
- Vivekananthan, Deepak P., et al. "Use of antioxidant vitamins for the prevention of cardiovascular disease: meta-analysis of randomised trials." The Lancet 361.9374 (2003): 2017-2023.
- Ye, Zheng, and Honglin Song. "Antioxidant vitamins intake and the risk of coronary heart disease: meta-analysis of cohort studies." European Journal of Cardiovascular Prevention & Rehabilitation 15.1 (2008): 26-34.
- Zhang, Sui-Liang, et al. "Effect of vitamin B supplementation on cancer incidence, death due to cancer, and total mortality: A PRISMA-compliant cumulative meta-analysis of randomized controlled trials." Medicine 95.31 (2016).
- Zourdos, Michael C., Marcos A. Sanchez-Gonzalez, and Sara E. Mahoney. "A brief review: the implications of iron supplementation for marathon runners on health and performance." The Journal of Strength & Conditioning Research 29.2 (2015): 559-565.