 |
| The only truly ergogenic addiction is a SuppVersity addiction ;-) |
Drug #1: Caffeine - From your coffee mug to the doping list
I am actually 100% confident that 99% of you have already trained "on drugs". Most of you probably do it regularly. Either with caffeine, about which Tony Chou reported in a 1992 paper that it is consumed on a daily basis by ~90% of the adult population (Chou. 1992). With average amounts of "only" 200 mg or 2.4 mg/kg/day (about 2 cups of coffee).
Why are you laughing? Caffeine was on the WADA's list of banned substances from 1962 to 1972 and again from 1984 to 2003. Whether the average coffee consumer will ever achieve concentrations of 12 μg/ml+ in the urine and thus fail a doping test is obviously a whole different question, but during the second banned period from 1984-2003, a whole host of athletes passed the magic 12 µg/ml line and were tested positive for caffeine. The sanctions ranged from warnings up to
2 year suspensions (maximum penalty, usually only 2–6 months; cf. Pesta. 2013).In view of the fact that its ergogenic effects are so well established as with hardly any other substance, I will stick to a very brief overview of the surprising benefits the world's "drug" #1 will have on preformance:
- Antagonism of adenosine ➲ analgesic effects (reduced perception of pain; Derry. 2012)
- Increased fatty acid oxidation ➲ higher endurance (Spriet. 1992)
- Decreased respiratory ration ➲ increased use of fat, decreased use of glycogen (Rush. 2001)
- Increases cAMP by inhibiting phospodiesterase ➲ increase lipolysis = more fuel (Umemur. 2006)
- Activation of protein kinase A ➲ s. above + increase in gluconeogenesis = more fuel (Graham. 2001)
- Increases glycogen storage ➲ faster recovery (Pedersen. 2008; learn more)
- Modulation of muscular calciusm flux ➲ increase contractile forces (Tarnopolsky. 2000)
Drug #2: Alcohol - From the track to the bar and into the gutter
While caffeine made it from everyone's coffee mug onto the WADA list of prohibited substances for all sports, alcohol is prohibited in-competition only and only in the following sports: aeronautic, archery, auto mobile, karate, motorcycling and powerboating (until 2010, modern pentathlon was also included in this list; Pesta. 2013).
Alcohol is a killer: According to WHO, morbidity attributable to alcohol in countries with an established market economy (10.3% of disability adjusted life years) comes second only to that of tobacco (11.7%; Murray. 1997). According to a very recent study by published in the scientific journal Addiction by the Pan American Health Organization, a branch of the World Health Organization alcohol was a 'necessary' cause of death (i.e., death would not have occurred in the absence of alcohol consumption) in an average of 79,456 cases per year in 16 North and Latin American countries (Gawryszewski. 2014).
In view of its effects on exercise performance and the generally reckless approach to the #2 on the list of the most diligent killers among all, not just the freely available drugs the decision of the World Anti Doping Association appears not reasonable, but at least consequent.For many cyclists at the Tour de France, it was common practice to drink one, two or three glasses, sometimes even a bottle of wine before during and after a race, but that was in the (good?) old days and its ergogenic effects are certainly questionable. Nevertheless, it took some time until the wine that was often laced with strychnine to help ease the pain and decrease the feeling of fatigue (Fife. 2000) got replaced by EPO, glucocorticoids & co [note: the cyclists also used cocaine or sympathomimetic drugs in order to attenuate the feeling of fatigue associated with such a prolonged exercise; cf. Lucia. 2003].
Now, aside from certain analgesic (=pain reducing) effects, alcohol has little to offer to the average athlete. It may still be the "the most commonly consumed drug in athletic communities" (Pesta. 2013), but in moderation and certainly not for ergogenic purposes.
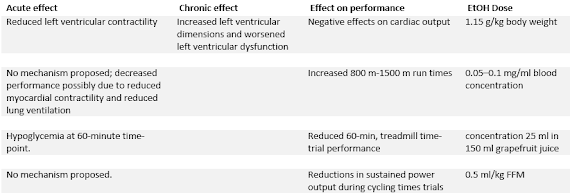 |
| Table 1: Summary of the effects of alcohol on performance (adapted from Pesta. 2013) |
 |
| Remember the irony in the article " Ultimate Post-Workout Testosterone Booze" [more] - Don't use hard liquor to increase your post-workout testosterone levels by almost 100%, unless figures on a lab report are more important to you than health & performance. |
- lead to significant impairments in cardiac and skeletal muscle structure and function in 99% of the cases
- slow down post-exercise recovery, and
- inhibit protein synthesis
Apropos health! I am sure all of you will be aware that the government of Colorado believes that marijuana should be part of a healthy lifestyle... ah, I mean medical protocol to deal with pain and other issues and decided to legalize the renown preparation of the Cannabis plant that's intended for use as a psychoactive drug and as medicine.
Drug #3: Cannabis, Mariuhana, Pot, Weed
As we have learned from the Tour de France athletes of the past, pain obviously is a major issue for athletes. So, wouldn't it make sense to switch from wine + strichnine to marijuana? Ok, you can't consume it "intra-workout", but maybe before and after the Queen's stage at L’Alpe d’Huez?!

- The centrally expressed CB1 receptors trigger the psychotropic effects of marijuana.
- The CB2 receptors in the periphery (spec. the sensory tissue) mediate the analgesic effects.
If these effects exist is yet probably almost as uncertain as the general usefulness of marijuana as an ergogenic, of which Pesta et al. write that if there were any, they would yet have to be established (Pesta. 2013).
- You don't have to smoke the weed to mess yourself up: Bird et al. demonstrated in 1980 that the previously mentioned detrimental effects on other aspects of performance occur with orally administered THC (215 µg/kg), as well. So don't even think of it ;-)Reduced work capacity of the heart at elevated heart rates -- Steadward and Singh (Steadward. 1971) were probably among the first scientists to test the effects of marijuana on exercise performance. In their study that was published as a dissertation at the University of Alberta in 1971 they found significant elevations in resting heart rate and both systolic and diastolic blood pressure at rest after marijuana consumption compared to both control and placebo. This lead to a highly significant decrease in physical work capacity at a heart rate of 170 (-25%)
- Decrease in time to exhaustion -- Renaud's and Cormier's finding from a 1986 study appear to confirm the earlier results Steadward and Singh present in their thesis paper. The researchers tested subjects 10 min after smoking a marijuana cigarette (containing 1.7% of Δ9-THC) of 7 mg/kg of body weight, and noted a slight, but significant decrease in cycle ergometry time to exhaustion. Avakian et al. [156] demonstrated that double.
If there even is a benefit for pot-heads, it's probably a psychological one that could be brought about by anxiety reducing and euphorigenic effects of cannabis... but let's be honest: Isn't a healthy amount of pre-competition anxiety a necessary prerequisite for world-class performance?
Drug #4: Nicotine - Better smoke tobacco than pot?
If alcohol doesn't help and pot is downright bad for you what else could you add to your beloved caffeine? Of course! Cigarettes. I mean, nicotine and caffeine that does even sound alike! Plus: Some "experts" say that they synergistically promote weight loss (which is a non-verified hypothesis that is often supported by a single short-term human trial by Jessen et al. (2003) and entails the risk of developing diabetes; cf. Attvall. 1993).
A note on different deliver routes: Both snus and nicotine gums enable nicotine to diffuse across the mucous membranes and are taken up by the bloodstream. The effects are yet still not necessarily identical to what we see, when it is inhaled and diffuses across the alveolar membrane - particularly if the source of the nicotine is a carcinogen-packed cigarette.
With its CNS stimulating and dopaminergic effects 3-(1-methyl-2-pyrrolidinyl)pyridine aka nicotine does at first appear to be a very likely candidate for every pre-workout supplement. Unfortunately, it does also enhance the effect of serotonin and opiate activity and will thus override its own stimulatory with a calming and depressing effect (Silvette. 1962). Against that background it sounds funny that nicotine will still increase the heart rate and blood pressure (Narkiewicz. 1998), as well as cardiac stroke volume and output and coronary blood flow (Bargeron. 1957). The question is thus: Which effects prevail? The stimulatory or the the sedating effects? The WADA apparently doesn't believe that nicotine doping is worth it. 3-(1-methyl-2-pyrrolidinyl)pyridine is currently on the watch list, but it's neither banned or officially tested for. That does yet not mean that it cannot yield small but significant benefits for endurance athletes (17% improvement in time to exhaustion in Mündel et al. 2006) or sports where dexterity / skills play an important role (improvement in the degree in a real-life motor task, Tucha et al. 2004; positive effect on fine-motor abilities, West et al. 1986; cf. Martin. 2009). None of these effects was observed with cigarettes, though, but with a 7mg nicotine patch, a 2mg nicotine chewing gum and 2mg intranasal nicotine, respectively.
 |
| Figure 1: Cigarette smoking and risk of diabetes among 41 810 men during six years follow up (Rimm. 1995) |
 |
| Nicotine + caffeine = heart damage, w/ and without ephedra | more |
If I had to pick my poison I would thus always go for caffeine and ignore alcohol, pot and even nicotine; and that in spite of the fact that the latter may exert (mainly neurological) benefits in certain sports.
- Anand, Praveen, et al. "Targeting CB2 receptors and the endocannabinoid system for the treatment of pain."Brain research reviews 60.1 (2009): 255-266.
- Attvall, S., et al. "Smoking induces insulin resistance—a potential link with the insulin resistance syndrome." Journal of internal medicine 233.4 (1993): 327-332.
- Burtscher, M., et al. "Motor symptoms similar to parkinsonism in heavy smokers." International journal of sports medicine 15.04 (1994): 207-212.
- Margeron, L., et al. "Effect of cigarette smoking on coronary blood flow and myocardial metabolism." Circulation 15.2 (1957): 251-257.
- Bird, K. D., et al. "Intercannabinoid and cannabinoid-ethanol interactions and their effects on human performance."Psychopharmacology 71.2 (1980): 181-188.
- Chopra, Gurbakhsh Singh. "Man and marijuana." Substance Use & Misuse 4.2 (1969): 215-247.
- Chou, Tony. "Wake up and smell the coffee. Caffeine, coffee, and the medical consequences." Western Journal of Medicine 157.5 (1992): 544.
- Derry, Christopher J., Sheena Derry, and R. Andrew Moore. "Caffeine as an analgesic adjuvant for acute pain in adults." Cochrane Database Syst Rev 3 (2012).
- Fife W, eds. Tour de France – The History, the Legend, the Riders, Vol. 100. Edinburgh and London: Mainstream Publishing, 2000: 1–255.
- Graham, Terry E. "Caffeine and exercise." Sports medicine 31.11 (2001): 785-807.
- Gawryszewski V.P., and Monteiro M.G. "Mortality from diseases, conditions, and injuries where alcohol is a necessary cause in the Americas, 2007-2009". Addiction (2014)[ahead of print].
- Jessen, Anna B., Søren Toubro, and Arne Astrup. "Effect of chewing gum containing nicotine and caffeine on energy expenditure and substrate utilization in men." The American journal of clinical nutrition 77.6 (2003): 1442-1447.
- Hill, Matthew N., et al. "Endogenous cannabinoid signaling is required for voluntary exercise‐induced enhancement of progenitor cell proliferation in the hippocampus." Hippocampus 20.4 (2010): 513-523.
- Lucia, Alejandro, Conrad Earnest, and Carlos Arribas. "The Tour de France: a physiological review." Scandinavian journal of medicine & science in sports 13.5 (2003): 275-283.
- Martin, Laura F., Deana B. Davalos, and Michael A. Kisley. "Nicotine enhances automatic temporal processing as measured by the mismatch negativity waveform." Nicotine & Tobacco Research 11.6 (2009): 698-706.
- Mündel, Toby, and David A. Jones. "Effect of transdermal nicotine administration on exercise endurance in men." Experimental physiology 91.4 (2006): 705-713.
- Murray, Christopher JL, and Alan D. Lopez. "Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study." The Lancet 349.9063 (1997): 1436-1442.
- Narkiewicz, Krzysztof, et al. "Cigarette smoking increases sympathetic outflow in humans." Circulation 98.6 (1998): 528-534.
- Pesta, Dominik H., et al. "The effects of caffeine, nicotine, ethanol, and tetrahydrocannabinol on exercise performance."Nutrition & metabolism 10.1 (2013): 71.
- Pedersen, David J., et al. "High rates of muscle glycogen resynthesis after exhaustive exercise when carbohydrate is coingested with caffeine." Journal of Applied Physiology 105.1 (2008): 7-13.
- Renaud, A.M., and Cormier, Y. "Acute effects of marihuana smoking on maximal exercise performance." Medicine and science in sports and exercise 18.6 (1986): 685-689.
- Rimm, Eric B., et al. "Prospective study of cigarette smoking, alcohol use, and the risk of diabetes in men." Bmj 310.6979 (1995): 555-559.
- Rush, James WE, and Lawrence L. Spriet. "Skeletal muscle glycogen phosphorylase akinetics: effects of adenine nucleotides and caffeine." Journal of Applied Physiology 91.5 (2001): 2071-2078.
- Silvette, H., et al. "The actions of nicotine on central nervous system functions." Pharmacological reviews 14.1 (1962): 137-173.
- Spriet, L. L., et al. "Caffeine ingestion and muscle metabolism during prolonged exercise in humans." American Journal of Physiology-Endocrinology And Metabolism 262.6 (1992): E891-E898.
- Steadward, R. D-, and Singh M. The effects of smoking marihuana on physical performance. Diss. University of Alberta, 1971.
- Stolerman, Ian P., and M. J. Jarvis. "The scientific case that nicotine is addictive." Psychopharmacology 117.1 (1995): 2-10.
- Taskinen, Marja-Riitta, and Ulf Smith. "Long-term use of nicotine gum is associated with hyperinsulinemia and insulin resistance." Circulation 94.5 (1996): 878-881.
- Tarnopolsky, Mark, and Cynthia Cupido. "Caffeine potentiates low frequency skeletal muscle force in habitual and nonhabitual caffeine consumers." Journal of applied physiology 89.5 (2000): 1719-1724.
- Tashkin, Donald P., et al. "Effects of smoked marijuana in experimentally induced asthma." Am Rev Respir Dis 112.3 (1975): 377-86.
- Tashkin, D. P., et al. "Cannabis, 1977." Annals of Internal Medicine 89.4 (1978): 539-549.
- Tucha, Oliver, and Klaus W. Lange. "Effects of nicotine chewing gum on a real-life motor task: a kinematic analysis of handwriting movements in smokers and non-smokers." Psychopharmacology 173.1-2 (2004): 49-56.
- West, R. J., and M. J. Jarvis. "Effects of nicotine on finger tapping rate in non-smokers." Pharmacology Biochemistry and Behavior 25.4 (1986): 727-731.
- Umemura, Takashi, et al. "Effects of acute administration of caffeine on vascular function." The American journal of cardiology 98.11 (2006): 1538-1541.