 |
| Don't be fooled. DHEA won't allow you to train forever day in and day out the study at hand does yet add to previous results which already suggested that it could have its merits whenever intensity and workloads are high (learn more) |
I see, guys, I got your full attention, now! And for the ladies, ...
... who may now believe that this article wasn't for them, I have a 2008 study from Steroids, one of the journals dealing with endocrine issues, which shows that DHEA is an important player in subcutaneous fat reduction in women (Hernandez-Morante. 2008), as well as a study in hypoadrenal women (any one suffering from the athlete's triad probably qualifies for self-induced hypoadrenalism, learn more) from Diabetes the journal of the American diabetes association showing profound improvements in insulin sensitivity after 12-weeks on 50mg/day DHEA. So don't click this article away, thoughtlessly, ladies!
 |
| 5x 1 min is obviously not the only sensible HIIT protocol. Read the SuppVersity Series on Making HIIT a HITand find out which HIIT-style would be right for you (learn more) |
This protocol was meant to shed some light unto the hitherto unknown effects of DHEA supplementation on testosterone levels during the recovery period after a bout of vigorous exercise. Interestingly, enough, you as a Suppersity addict (or soon to be addict ;-) will be aware that DHEA's beneficial effects on recovery in general have actually been proven - even in a scenario of temporary overreachig (=strategic overtaining for a short time period to elicit a maximal training stimulus; see figure 1 and read all the details in my May 2012 article).
 |
| Figure 1: Changes in DHEA-S serum levels and exercise induced elevations of creatine kinase =marker of muscle damage) in 16 healthy untrained college aged men receiving 100mg/day DHEA or placebo during a 5-day "mixed-type exercise" regimen (this graph was originally discussed on May 27, 2012 and is based on Liao. 2013) |
 |
| Figure 2: Dehydroepiandrosterone (DHEA-S) and total testosterone levels (TT) during the interention; the asterisk (*) over the TT bars signifies significantly different from placebo in the same age group (Liu. 2013) |
"Nice, but where's the data on cortisol and what about free test & LH?"
What is not shown in figure 1 are the cortisol levels of the study participants, which were not significantly different at baseline. After the exercise intervention, the levels did yet increase significantly - irrespective of whether or not the participants were young or middle aged or received the placebo or the actual DHEA pills. Intriguingly, the drop that occured after 24h in both age groups was much more pronounced in the middle-aged guys.
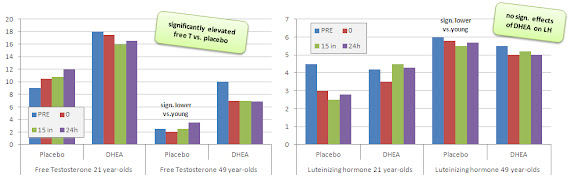 |
| Figure 3: Free testosterone and luteinizing hormone levels during the intervention (Liu. 2013) |
"[...] the free testosterone to cortisol [FT/C] ratio increased significantly during the training recovery for both the middle-aged and young control groups." (Liu. 2013)Now all that is good news, but what's even better news is that, at least in the short run, these profound elevations in free testosterone did not lead to lower levels of the "testosterone production trigger" luteinizig hormone (LH), which is released by your hypothalamus and tells your testes to produce more sex hormones. Now why is that important? Well, the answer is simple, a reduction in LH is not just a sign of the dreaded HTPA shut-down, it is the shutdown - or I should say the mechanistic cause of being "shut down" (=not producing any or too little sex hormones on your own).
Ok, higher T levels, lower testosterone to cortisol ratio, but what about estrogen?
A note on performance and estrogenic side-effects: An 8-week exercise intervention by Brown et al. which used 50mg DHEA /day combined with 3x total body workouts per week did not produce significant changes in any of the study parameters. Neither beneficial ones, such as greater strength increases or hypertrophy, nor negative ones such as increases in estrogen or deteriorations of the lipid profile (Brown. 1999). In 2010, on the other hand, Ostojic et al. reported that 4 weeks of 100mg DHEA, despite having no effects on the body composition of the 19-21 year-old soccer players who participated in the study, led to statistically significant increases in total testosterone (+37%), DHEA-S (+197%) and estradiol (+21% compared to the subjects in the placebo group; Ostojic. 2010). The overall significance of these results is yet questionable, since both studies were pretty underpowered (N=10 and N=20 for Brown and Ostojic, respectively). It is still noteworthy that the DHEA induced "estrogen dominance", which is one of the most frequenly heardt arguments against DHEA supplementation was not observed in either of the two studies.
If the above is the question that's just praying on your mind, then this is probably not the first article on DHEA administration you've read and what's more, the other ones were probably not published on the SuppVersity. While it is true that a handful of previous studies have in fact shown an increase of estrogen in response to the administration of DHEA, the important ratio of testosterone to estrogen was maintained even in the majority of those studies, where this effect was observed (for more details read the text in the red box on the right). Regardless of how "real" the danger of elevated estrogen levels may be, there is actually another way more important question to be answered, which pertains to the sustainability of the results. In view of the fact that the DHEA was only administered once, it is way more likely that the unquestionably beneficial effects the scientists observed could be of very transient / short-lived nature. The minimal changes in luteinizing hormone for example could well become significant (and negative) in the long run. After all a +100% increase in free testosterone is nothing your body is going to ignore for weeks. It's more likely that it will slowly bounce back to the former steady state by either reducing the production of testosterone or that of DHEA.
So even if it's unlikely that the small dosage of 50 mg would eventually shut you down, you may well lose the benefits after one months of continuous supplementation.
That being said, you could also argue that the exogenous DHEA has, just as TRT or performance enhancing drugs, the advantage of not being subject to diet-, training- and obviously age-induced reductions in their endogenous production. If any of the latter reminds of a situation / period of your life you are in, your chances of seeing benefits would at least be higher - whether they would be high enough to actually manifest in beneficial training outcomes remains questionable, though.
 |
| It is unfortunate that science gave up on DHEA, when it became clear that it's not the fountain of youth. I mean, greater fat-inhibition effects than testosterone are nice, no (learn more about those)? |
Unfortunately, the evidence from these short-term interventions does not tell us anything about the beneficial and detrimental effect the low and high dose protocols from the Liuand the Liao studies will have. Personally I would assume that the benefits will wane off, but in the absence of corresponding studies, this is mere guesswork. After all, 99% of the previous research on DHEA has been done in sedentary old men and women. Few trials investigated the effects on young or middle aged subjects and less than a handful did that in an exercise scenario with any resemblances to yours or mine.
So there is probably need for at least another SuppVersity article (obviously based on a novel study), before you will hear me recommend the use of DHEA as an ergogenic supplement. Now, if you want to make sure, you don't miss that, I suggest you start following the SuppVersity on Facebook, Twitter or simply with your favorite RSS reader (click here to get to the channel ;-)
References:
- Brown GA, Vukovich MD, Sharp RL, Reifenrath TA, Parsons KA, King DS. Effect of oral DHEA on serum testosterone and adaptations to resistance training in young men. J Appl Physiol. 1999 Dec;87(6):2274-83.
- Hernández-Morante JJ, Pérez-de-Heredia F, Luján JA, Zamora S, Garaulet M. Role of DHEA-S on body fat distribution: gender- and depot-specific stimulation of adipose tissue lipolysis. Steroids. 2008 Feb;73(2):209-15.
- Labsy Z, Prieur F, Le Panse B, Do MC, Gagey O, Lasne F, Collomp K. The diurnal patterns of cortisol and dehydroepiandrosterone in relation to intense aerobic exercise in recreationally trained soccer players. Stress. 2013 Mar;16(2):261-5.
- Liao YH, Liao KF, Kao CL, Chen CY, Huang CY, Chang WH, Ivy JL, Bernard JR, Lee SD, Kuo CH. Effect of dehydroepiandrosterone administration on recovery from mix-type exercise training-induced muscle damage. Eur J Appl Physiol. 2013 Jan;113(1):99-107.
- Liu TC, Lin CH, Huang CY, Ivy JL, Kuo CH. Effect of acute DHEA administration on free testosterone in middle-aged and young men following high-intensity interval training. Eur J Appl Physiol. 2013 Feb 17.
- Oskis A, Clow A, Thorn L, Loveday C, Hucklebridge F. Differences between diurnal patterns of salivary cortisol and dehydroepiandrosterone in healthy female adolescents. Stress. 2012 Jan;15(1):110-4.
- Ostojic SM, Calleja J, Jourkesh M. Effects of short-term dehydroepiandrosterone supplementation on body composition in young athletes. Chin J Physiol. 2010 Feb 28;53(1):19-25.
- Thuma JR, Gilders R, Verdun M, Loucks AB. Circadian rhythm of cortisol confounds cortisol responses to exercise: implications for future research. J Appl Physiol. 1995 May;78(5):1657-64.