 |
| Fat is an important nutrient for the unborn child. Accordingly, the question is not if pregnant women should consume fat, it's rather how much and at which ratios saturated, monounsaturated (MUFA) and polyunsaturated (PUFA) fatty acids should be consumed. A new study does now go even one step further and tries t assess the optimal amount of individual fatty acids like arachidonic acid (ARA), Eicosapentaenoic acid (EPA) or Docosahexaenoic acid (DHA). |
As you will probably know, a high-intake ratio of n -6/n-3 polyunsaturated fatty acids (PUFAs) has been suggested to contribute to excess fetal adipose tissue development - a hypothesis that is, as Alihaud et al. pointed out in their 2004 review, "supported by epidemiological data from infant studies as well as by the assessment of the fatty acid composition of mature breast milk and formula milk" and allegedly a consequence of the fact that n6 fatty acids are "potent promoters of both adipogenesis in vitro and adipose tissue development in vivo" (Alihaud 2004).
High-protein intakes during pregnancy are linked to higher lean mass (Tielemans 2016).

Practical Protein Oxidation 101

5x More Than the FDA Allows!

More Protein ≠ More Satiety

Protein Oxidation = Health Threat

Protein Timing DOES Matter!

Keto for Superior Weight Loss?
"An enhanced maternal-fetal n−3 PUFA status was associated with lower childhood adiposity."
The problem, however, is that this conclusion is based on a cohort of which we all know that it is chronically deficient in N-3 fatty acids and laden with pro-inflammatory N-6s - the American Diet. Since you're not stupid enough to believe that N3s are good, while N6s are bad, you will also know that perfect health in adults, babies and even unborns will not be achieved by avoiding one and consuming another essential nutrient in excess (the n-6/n-3 ratio in the Donahue study is 12:1, in the more recent study by Hakola et al. that's based on the Finnish birth cohort with 3807 mother–child pairs it is 10:3, i.e. 58% lower).
Why is modeling better than linear analysis? If we talk about the effects of foods, behavior, and whatnot on our weight, health, or other parameters, it is unrealistic to assume that the relationship between, say, food intake and health outcome X is linear. Rather than that it seems logical to assume that it is U-shaped with a happy medium and problems resulting from both, eating too much and too little food. The statistical analysis of the data from Hakola et al. (2017) can identify these relationships, the multivariate linear analysis in Daonahue (2011) can not.
 |
| Figure 1: It is important not to forget the really important modulators of your kids' obesity risk for boys (1st) and girls (2nd value): your BMI, how much weight you gain during pregnancy (keyword: piggin' out), and highly correlated your child's birth weight (data based on Hakola 2017). |
"[...] generalized estimating equation (GEE) models [were used] to study the associations of covariates and maternal dietary variables on the repeatedly measured offspring overweight and obesity[; an] autoregressive working correlation structure was used to model the correlation of the repeated outcomes" (Hakola 2017).Furthermore, Hakola et al. (2017) conducted separate analysis for boys and girls and tracked the children from year 2-7 and thus beyond the 3-year mark of the Donahue study.
 |
| Low EPA and high ARA are obesity protective according to Hakola 2017. |
- In girls, maternal intake ratio of n-6:n-3 PUFAs had a U-shaped association with obesity (adjusted OR for the lowest 2.0 [95% CI 1.27–3.20] and the highest 1.7 [1.03–2.73] vs. the two middle quartiles of n-6:n-3 PUFAs, p = 0.01).
- In boys, arachidonic acid (20:4n-6): docosahexaenoic acid + eicosapentaenoic acid ratio was associated with obesity (adjusted OR for the lowest 1.0 [0.60–1.57] and the highest 0.5 [0.26–0.88] vs. the two middle quartiles, p = 0.02).
- Saturated fatty acids and monounsaturated fatty acids were not associated with overweight or obesity in either sex.
In girls, the n-6/n-3 ratio showed a U-shaped relationship w/ obesity; in boys avoiding n-6s and thus their long-chain variety arachidonic acid while prioritizing DHA+EPA (n-3) will even increase the boys' risk of overweight and obesity at age 2-7 by 50%!
That there's a sex-difference with respect to the pro-/anti-obesity effects of dietary fat consumption during pregnancy has been known for years, the specificity for certain fatty acids, on the other hand, is a novel result - just like the nonlinearity of the link between the n-6-to-n-3 ratio and its effects on overweight/obesity in girls (the data for linoleic acid/linolenic acid is virtually identical).
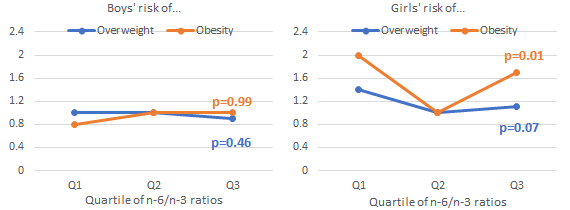 |
| Figure 2: Overweight and obesity risk according to quartiles (the higher the quartile, the greater the ratio) of n-6/n-3 intakes in male (left) and female (right) offspring; based on Finnish birth cohort (3807 mother–child pairs; Hakola 2017). |
...unfortunately, I cannot tell you the exact optimal numbers, because it was neither in the full text of the study nor in the supplemental data.
Now that may sound "bad", but an "optimum" calculated based on a single prospective study that was conducted in a country you don't even live in (my Finnish friends: please ignore the last argument, but acknowledge that a single study cannot identify the "optimum", anyway).
 |
| Figure 3: Overweight and obesity risk according to quartiles of arachidonic acid (ARA) to DHA+EPA ratio in male (left) and female (right) offspring; based on Finnish birth cohort (3807 mother–child pairs; Hakola 2017) |
 |
| Figure 4: The metabolic processing and effects of n-6 and n-3 metabolism on selected exemplary physiological processes ranging from inflammation and immunity to vascular and brain health (Uauy 2006). |
Yes, DHA and EPA are healthy, yes, they are essential (at least for mothers to be / their unborn offspring), and yes, they are a deficiency nutrient in the average western diet. That a given nutrient is healthy and essential, however, does not imply that its physiological/nutritional counterpart is unhealthy and non-essential. Both, N3- and N-6 fatty acids are essential for the normal development of unborn babies.
It is thus hardly surprising that the study at hand emphasizes the importance of ratios and the inadequacy of the assumption that the link between the n-6/n-3 ratio and/or individual fatty acids was necessarily linear.
It would be a huge mistake to use the data from the study at hand to estimate "optimal" intakes for mothers, for at least three reasons: Firstly, we are (a) talking about a single study, even if it was the perfect study, that wouldn't be enough to make reliable general statements. Secondly, the study was (b) conducted in a population that has one of the highest intakes of plant n-3 PUFAs in the world and an above average intake of seafood n-3 PUFAs (Pietinen 2010; Micha 2014). Women from Finland and a country like the US will thus differ not only with respect to their fatty acid intakes but also with respect to the levels of n-6s and n-3s in their blood and cells. It is thus not surprising that US-studies like Donahue et al. (2011) found inverse linear associations between n-3 intakes and childhood weight that turned out to be U-shaped in the Hakola study, with subjects with significantly higher n-3 intakes. Third- and lastly, childhood obesity is (c) a huge problem and contributes to the diabesity epidemic with all its unhealthy consequences, it is yet by no means the only factor we'd have to consider if we wanted to recommend "optimal" ratios for n-6/n-3 and, more specifically, ARA/DHA+EPA intakes in pregnant women.
What we can already say with some certainty is that mothers-to-be should consume a balanced diet, a diet that contains both, n-6 and n-3 fatty acids in a ratio that cannot be determined based on the limited database we have, today - a ratio that will probably differ according to at least three parameters: offspring sex, maternal baseline diet, and, obviously, the health parameter we're looking at (e.g. obesity at age 2-7 vs. IQ at age 2-7 vs. insulin sensitivity, etc.) | Comment!
- Ailhaud, G., and P. Guesnet. "Fatty acid composition of fats is an early determinant of childhood obesity: a short review and an opinion." Obesity reviews 5.1 (2004): 21-26.
- Donahue, Sara MA, et al. "Prenatal fatty acid status and child adiposity at age 3 y: results from a US pregnancy cohort." The American journal of clinical nutrition 93.4 (2011): 780-788.
- Hakola, L., Takkinen, H-M., Niinistö, S., Ahonen, S., Erlund, I., Rautanen, J., Veijola, R., Ilonen, J., Toppari, J., Knip, M., Virtanen, S. M., and Lehtinen-Jacks, S. "Maternal fatty acid intake during pregnancy and the development of childhood overweight: a birth cohort study." Pediatric Obesity 12 (2017): 26–37. doi: 10.1111/ijpo.12170.
- Micha, Renata, et al. "Global, regional, and national consumption levels of dietary fats and oils in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys." Bmj 348 (2014): g2272.
- Pietinen, Pirjo, et al. "FINDIET 2007 Survey: energy and nutrient intakes." Public health nutrition 13.6A (2010): 920-924.
- Simopoulos, Artemis P., and Norman Salem. "Egg yolk as a source of long-chain polyunsaturated fatty acids in infant feeding." The American journal of clinical nutrition 55.2 (1992): 411-414.
- Tielemans, Myrte J., et al. "Protein intake during pregnancy and offspring body composition at 6 years: the Generation R Study." European journal of nutrition (2016): 1-10.
- Uauy, Ricardo, and Alan D. Dangour. "Nutrition in brain development and aging: role of essential fatty acids." Nutrition reviews 64.s2 (2006).