 |
| While milk with honey is better than milk with glucose (Jalilolghadr 2011), it won't improve - if anything mess - with your sleep quality when it's consumed ≤ 1h before bedtime - noteworthy: the same goes for most foods, though. |
That's in contrast to a number of supplements that are discussed in a recent review by scientists from the Northwestern University; a review that highlights both, the short-comings of the existing research on dietary supplements for insomnia and encourage health practitioners "to explore existing resources and partner with patients to understand their goals and advise on safe and effective use of dietary supplements" (Ring 2017).
Studies related to sleep and sleep supplements at the SuppVersity:

Sleep Like an Athlete!

Phenibut Addic- tive or Harmless?
 All About GABA at SHR
All About GABA at SHR
Melatonin = Easy Fat Loss?

Letrozole? Use Melatonin Instead

Bone & Tooth? Melatonin Helps
- Valerian - The probably most prominent and certainly one of the best-researched natural sleep aid is the root of Valeriana officinalis - a sleep aid that works... for some.
Since "[v]alerian and its constituent valerenic acid have demonstrated adenosine (A1 receptor) interactions, GABAA receptor (β3 subunit) agonism, and 5-HT5a partial agonism" (Ring 2017) it may be surprising that only 6/9 studies in a recent review by Bent et al showed no effect on subjective sleep quality.
In addition, Bent et al (2006) highlight that "[m]ost studies had significant methodologic problems, and the valerian doses, preparations, and length of treatment varied considerably". More recently, a meta-analysis by concluded:![]()
Figure 1: Likelihood that valerian improved sleep quality calculated based on Meta-analysis of 6 studies reporting dichotomous outcomes for sleep quality (adapted from Bent et al. 2006). "The qualitative dichotomous results suggest that valerian would be effective for a subjective improvement of insomnia, although its effectiveness has not been demonstrated with quantitative or objective measurements. Nevertheless, its use can be considered for some patients given its safety" (Fernández-San-Martín 2010).
Objective evidence for the efficacy of valerian is thus still missing... possibly due to the use of low-dose / low-concentration supplements. Speaking of which... here are the dosage suggestions Ring et al. provide in their previously cited review.
Dosage: It seems as if it took at least 300–900 mg of a standardized extract of 0.8% valerenic acid - the dosage Ring et al. recommend as an alternative for valerian tea (1.5–3 g of root steeped for 5–10 min in 150 mL of boiling water) - to be taken 30–120 min before bedtime. Effects seem to accumulate over time and may not be noticed with the first administration.

High saturated fat intakes linked to less recuperative slow-wave sleep: In their 2016 study, a randomized crossover inpatient study with 2 phases of 5 nights, St Onge et al. observed differential effects of high fiber and high saturated fat intakes on slow-wave sleep While greater fiber intakes predicted less stage 1 (P = 0.0198) and more SWS (P = 0.0286), the percent of energy from saturated fat predicted less SWS (P = 0.0422).
- Hops - In (non-alcoholic) beer, hops seems to work wonders for some of us... but wait a minute: is that actually the small quantity of 2-methyl-3-buten-2-ol, xanthohumol, and myrcenol from Humulus lupulus and its effect on GABA that's responsible for these effects?
The fact that non-alcoholic beer works (note: the alcohol in regular beer will reduce REM and boost SWS, but it will also mess w/ the nightly growth hormone production | Prinz 1980), as well, would suggest that it's at least not the alcohol that's responsible for the improvements in subjective sleep quality (assessed by questionnaires), decrease in sleep latency (=time it takes you to fall asleep), and improvement of overall global score of sleep quality improved (Franco 2012 & 2014).
On the other hand, the fact that hops extracts didn't yield comparably convincing results would suggest that there's more to beer than hops and/or the brewing process gives rise to metabolites that are driving an efficacy that cannot be achieved with commercial hops extracts - extracts that have, in contrast to the non-alcoholic beer, been tested in people with chronic insomnia. It is thus not clear if it's the preparation or the subject group (or both) that's responsible for the mixed results of hops only preparations (evidence in favor of valerian + hops combinations is more promising - even in insomniacs).![]()
Figure 2: We better stay skeptical about the role of hops in the beneficial effects of non-alcoholic beers as it has been observed by Franco et al. in stressed Hungarian students in 2014. It's well possible that it's just the carb content of the beer that triggered the improvements in sleep latency and quality in Franco et al. (2014).
Dosage: Unlike valerian and most of the other agents discussed in this overview, hops is not without side effects. When administered in high(er) dosages (HED ~64mg/kg) to mice in conjunction with ketamine, the mice resulted in a deep narcosis. For me, that's another reason to rather drink 300ml of a (non-alcoholic) beer with dinner (check out other health benefits of beer) than to take 120–400 mg of hop extract (ideally combined with 374–500 mg of valerian root extract) to up your sleep quality. Immediate effects can be expected.

|
| Blindfolds and earplugs can improve your sleep quality significantly and help resynchronize a messed up circadian rhythm, which is important for both average Joes and athletes | learn more about "Sleeping like an athlete" in my article from June 2017! |
It is thus not really surprising that studies have shown that, after REM sleep loss, procedural memory and motor skills can be affected (Stickgold and Walker 2007). Another relevant physiological phenomenon for athletes is the blockade of cortico-spinal pathways at the brain stem and subsequent suppression of motor activity, which induces a state of total muscle relaxation "that allows effective myofibril restoration" (Davenne 2009).
- Cherries (esp. tart cherries) - Cherries are well-known for their l-tryptophan content, if you fast forward to the corresponding section of this article it is thus not surprising that cherries/cherry-juice seems to be a highly promising sleep quality modulator.
Next to the serotonin- and melatonin-precursor l-tryptophan, cherries contain a plethora of anti-oxidants, as well as pre-formed melatonin - a cocktail that may well explain why a randomized, double-blind, crossover study on the effect of tart cherries on older adults (age ≥ 65 years) with insomnia found that the consumption of an 8-oz serving of tart cherry juice twice daily for 2 weeks found a statistically significant reductions in insomnia severity (measured as minutes awake after sleep onset).
Moreover, another study in 20 healthy men and women (aged 18 to 40), which detected significant elevations in urinary melatonin, confirms that the benefits are not restricted to the elderly population in whom the natural production of melatonin is known to decrease. After all, the increase in melatonin Pigeon et al. detected in the urine of the subjects, who complained of insomnia but were otherwise healthy, came with significant increases in time in bed, total sleep time, and sleep efficiency (Pigeon 2010).![]()
Figure 3: Plot of the relative changes in selected markers of sleep quality; p-values for time x group effects indicate statistical significance for insomnia index and wake after sleep onset (Pigeon 2017).
Dosage: While pills are available, all promising research has been done using (tart) cherry juice (8 oz consumed 2x per day, chronically). Compared to whole fruits, the juices also have the advantage of being easier to stomach than the significant number of cherries you'd have to consume to get remotely close to the concentration of active ingredients in the currently available proprietary tart cherry drinks. Immediate effects cannot be expected.

Very low-carb and ketogenic diets shift the ratio of SWS to REM sleep in favor of the former: Whether it is a good or bad thing that Afaghi et al. (2008) observed a significant reduction in REM and a corresponding increase in slow-wave sleep (SWS) is still in the open. What is certain, though, is that (a) low-fat high-carb diets have previously been shown to have the opposite effect (Phillips 1975) and that (b) the pro-SWS effects of ketogenic diets can be used in the treatment of abnormal refractory continuous spikes and waves during slow sleep (Nikanorova 2009).
- L-tryptophan - The serotonin and melatonin precursor may actually help you fall asleep and stay asleep, but the # of studies is limited.
Intriguingly, much of the existing evidence of tryptophan's efficacy is >35 years old, with a review by Ernest Hartmann (1982) highlighting three things- "the weight of evidence indicates that L-tryptophan in doses of 1 g or more produces an increase in rated subjective sleepiness and a decrease in sleep latency (time to sleep)",
- "there are less firm data suggesting that L-tryptophan may have additional effects such as decrease in total wakefulness and/or increase in sleep time", and
- "negative results occur in entirely normal subjects—who are not appropriate subjects since there is 'no room for improvement'"
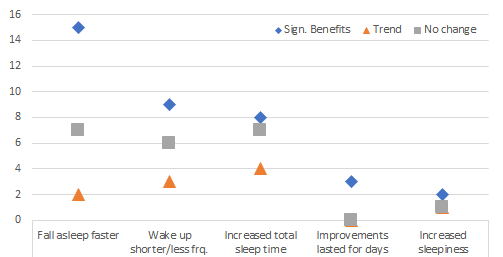
As my plot of the number of studies showing significant benefits, trends and no effects highlights, a reduced sleep latency is what appears to be the most certain benefit you can get from 1g+ of l-tryptophan taken ~30 minutes before bed. Potential benefits may be seen from the same regimen (for the # of occasions you wake up and/or toss and turn, as well as the total sleep time.![]()
Figure 4: Graphical illustration of the number (N=y) of studies showing significant, benefits, trends or no change according to a 1982 review in the Journal of Psychiatric Research by Ernest Hartmann (1982)
Dosage: No clear benefits have been observed for higher dosages (even though studies tested boluses of up to 15g), but it seems advisable especially for lower dosages to consume them "on empty", i.e. at least without other protein foods. Effects - at least the sleepiness - may be expected with the first administration.
High GI-carbs significantly speed up (-49%) how long it will take you to fall asleep: While high GI carbs (GI = 109) still have a bad rep, studies indicate that consumed 4h before bed will speed up the sleep latency of healthy individuals by a whopping 49% (9.0 ± 6.2 min vs. 17.5 ± 6.2 min for otherwise identical low-GI meals (GI =50) | Afaghi 2007)... to consume the meal 4h before bed is important, by the way. In the same study, Afaghi et al. observed that the same meal given 1 h before bedtime increased the sleep latency back to 14.6 ± 9.9 minutes. Other studies even suggest detrimental effects with high GI ingestion too close to bedtime (so stick to the 4h) - including milk + glucose (higher GI) vs. the notorious milk + honey mix (lower GI) when consumed ~60 minutes before bed.
General beneficial effects of carbs have been observed, among others, by Porter and Horne (1981) who provided six male subjects with a high-carbohydrate meal (130 g), a low-carbohydrate meal (47 g), or a meal containing no carbohydrate, 45 min before bedtime. The high-carbohydrate meal resulted in increased REM sleep, decreased light sleep, and wakefulness. As Halson et al. (2014) point out in their review, "the caloric content of the meals was [yet] not matched in the study".
General beneficial effects of carbs have been observed, among others, by Porter and Horne (1981) who provided six male subjects with a high-carbohydrate meal (130 g), a low-carbohydrate meal (47 g), or a meal containing no carbohydrate, 45 min before bedtime. The high-carbohydrate meal resulted in increased REM sleep, decreased light sleep, and wakefulness. As Halson et al. (2014) point out in their review, "the caloric content of the meals was [yet] not matched in the study".
- l-theanine - Usually supplements that are so heavily advertised as Just Chill™ and NeuroSleep™ don't work, but for these l-theanine things could be different.
As the authors of the previously cited review in Current Sleep Medicine Reports point out in their review, "[s]everal studies have shown that intake of L-theanine significantly increases α-wave activity in different areas of the cerebral cortex, leading to a relaxed state without drowsiness" (Ring 2017).
In conjunction with its ability to increase dopamine and serotonin, and reduce stress-related norepinephrine and cortisol levels, salivary IgA, and heart rate in response to an acute stressor. Plus: L-theanine has been shown in animal studies to partially reverse caffeine-induced reductions in slow wave sleep (Jang 2012) - effects that can occur even with your average morning Joe (i.e. not just with caffeine consumption late in the day | Landolt 1995).![]()
Figure 5: 200mg/day l-theanine reduce the cortisol release in response to stress (Kimura 2007).
The reason why I still used "could" in the headline of this paragraph is that there is, more or less, only one convincing study to demonstrate beneficial effects on sleep quality in human beings: a 2011 study by Lyon et al. that investigated the effects of Suntheanine® (a branded l-theanine product) on objective sleep quality in boys with attention deficit hyperactivity disorder (ADHD) and showed objective (actigraph) improvements in sleep percentage and sleep efficiency after 6 weeks.
Similar objective improvements in sleep efficiency and intermittent awakening (WAS) are also reported by Rao et al. (2015) for healthy subjects (see Figure 6).![]()
Figure 5: . (a) Sleep length, (b) sleep efficiency, and (c) intermittent awakening WASO data interpreted from actigraph measurements in 10 male subjects. The values represent mean § standard error. Statistical significance was measured using Student’s paired t-test (Rao 2015).
Dosage: While you will see recommendations ranging from 50 to 400 mg of L theanine taken 30–60 min before bedtime, the "proven" dosage is 200mg. That's more than 4 cups of high l-theanine green tea and thus not really achievable by consuming freshly brewed green tea before bed. As Ring et al. point out, you have to be careful, though, because "[l-t]heanine can have an antihypertensive effect, so it should be used with caution when combined with antihypertensive medications" (Ring 2017). - Melatonin - Your body's own sleep aid is rather a circadian re-aligner than a true sleeping pill - that's why it works mostly for problems with falling asleep.
The decrease in sleep onset latency can but doesn't necessarily result in increases in total sleep time. That's why many users who expected benzo-esque results are disappointed.
On the other hand, melatonin has none of the nasty side effects of your average BZD-Z drugs: memory and cognition impairment, psychomotor retardation, or next-day hangover effects (if dosed correctly | Wilson 2010). Likewise, an often-heard of physical dependence has never been observed (Zhdanova 1996).
Dosage: Dosing melatonin is difficult because the optimal dosage differs between individuals. Accordingly, Ring et al. (2017) suggest a dosage plan starting with 0.3mg and increasing to 3mg (max. 6mg) if the desired effects don't occur.
.


 |
| Two Hours of Extra-Sleep Before Sleep Deprivation Minimize the Performance Decrements Due to 24h Sleep Deprivation | more |
Experimentation may be necessary to find out what works for you - one-size-fits-it-all advice is unwarranted!
The above is especially true for melatonin, which didn't make the A-list, because it's more of a circadian re-aligner than a sleep aid. This doesn't make it less useful, though - on the contrary: if used correctly (1-2h before bed at 0.3-6.0 mg depending on your tolerance) it can have far-reaching beneficial effects on both, your sleep latency, quality, and duration as well as your overall health.
What neither melatonin nor any other sleep aid can make up for, though, is sleep hygiene.
One supplement that has evidence to support its effect, which I still won't recommend, though, is (*) Kava Kava (Piper methysticum), which messes w/ the cytochrome enzyme cascade (CYP450), will affect the metabolism of both meds and other dietary supplements, and has been linked to liver failure (albeit outside of RCTs lasting up to 6 months | Clouatre 2004), as well as the following concoctions that are often recommended but don't have convincing scientific backup: (i) chamomile, despite proven interactions of apigenin in chamomille w/ the GABA receptor, (ii) passion flower, (iii) California poppy, (iv) skullcap, (v) lemon balm, (vi) St. John’s wort, (vii) lavender, and (viii) magnolia bark | Comment on Facebook!
References:
- Afaghi, A., O'connor, H., & Chow, C. M. (2007). High-glycemic-index carbohydrate meals shorten sleep onset. The American journal of clinical nutrition, 85(2), 426-430.
- Afaghi, A., O'Connor, H., & Chow, C. M. (2008). Acute effects of the very low carbohydrate diet on sleep indices. Nutritional neuroscience, 11(4), 146-154.
- Bent, S., Padula, A., Moore, D., Patterson, M., & Mehling, W. (2006). Valerian for sleep: a systematic review and meta-analysis. The American journal of medicine, 119(12), 1005-1012.
- Clouatre, D. L. (2004). Kava kava: examining new reports of toxicity. Toxicology letters, 150(1), 85-96.
- Davenne, Damien. (2009) "Sleep of athletes–problems and possible solutions." Biological Rhythm Research 40.1: 45-52.
- Dement, W C. (2005). "Sleep extension: getting as much extra sleep as possible." Clinics in Sports Med, 24: 251–268.
- Fernández-San-Martín, M. I., Masa-Font, R., Palacios-Soler, L., Sancho-Gómez, P., Calbó-Caldentey, C., & Flores-Mateo, G. (2010). Effectiveness of Valerian on insomnia: a meta-analysis of randomized placebo-controlled trials. Sleep medicine, 11(6), 505-511.
- Franco, L., Sánchez, C., Bravo, R., Rodríguez, A. B., Barriga, C., Romero, E., & Cubero, J. (2012). The sedative effect of non-alcoholic beer in healthy female nurses. PloS one, 7(7), e37290.
- Franco, L., Bravo, R., Galán, C., Rodríguez, A. B., Barriga, C., & Cubero, J. (2014). Effect of non-alcoholic beer on Subjective Sleep Quality in a university stressed population. Acta Physiologica Hungarica, 101(3), 353-361.
- Halson, S. L. (2014). Sleep in elite athletes and nutritional interventions to enhance sleep. Sports Medicine, 44(1), 13-23.
- Hartmann, Ernest. "Effects of L-tryptophan on sleepiness and on sleep." Journal of psychiatric research 17.2 (1982): 107-113.
- Jalilolghadr, S., Afaghi, A., O'Connor, H., & Chow, C. M. (2011). Effect of low and high glycaemic index drink on sleep pattern in children. JPMA-Journal of the Pakistan Medical Association, 61(6), 533.
- Jang, H. S., Jung, J. Y., Jang, I. S., Jang, K. H., Kim, S. H., Ha, J. H., ... & Lee, M. G. (2012). L-theanine partially counteracts caffeine-induced sleep disturbances in rats. Pharmacology Biochemistry and Behavior, 101(2), 217-221.
- Kimura, K., Ozeki, M., Juneja, L. R., & Ohira, H. (2007). L-Theanine reduces psychological and physiological stress responses. Biological psychology, 74(1), 39-45.9
- Landolt, H. P., Werth, E., Borbély, A. A., & Dijk, D. J. (1995). Caffeine intake (200 mg) in the morning affects human sleep and EEG power spectra at night. Brain research, 675(1), 67-74.
- Lyon, M. R., Kapoor, M. P., & Juneja, L. R. (2011). The effects of L-theanine (Suntheanine®) on objective sleep quality in boys with attention deficit hyperactivity disorder (ADHD): a randomized, double-blind, placebo-controlled clinical trial. Alternative medicine review, 16(4), 348.
- Ozeki, Makoto, Lekh Raj Juneja, And Shuichiro Shirakawa. "The Effects Of L-Theanine On Sleep Using The Actigaph." Japanese Journal Of Physiological Anthropology 9.4 (2004): 143-150.
- Nikanorova, M., Miranda, M. J., Atkins, M., & Sahlholdt, L. (2009). Ketogenic diet in the treatment of refractory continuous spikes and waves during slow sleep. Epilepsia, 50(5), 1127-1131.
- Phillips, F., Crisp, A. H., McGuinness, B., Kalucy, E. C., Chen, C. N., Koval, J., ... & Lacey, J. H. (1975). Isocaloric diet changes and electroencephalographic sleep. The Lancet, 306(7938), 723-725.
- Pigeon, W. R., Carr, M., Gorman, C., & Perlis, M. L. (2010). Effects of a tart cherry juice beverage on the sleep of older adults with insomnia: a pilot study. Journal of medicinal food, 13(3), 579-583.
- Porter, J. M., & Horne, J. A. (1981). Bed-time food supplements and sleep: effects of different carbohydrate levels. Electroencephalography and clinical neurophysiology, 51(4), 426-433.
- Prinz, P. N., Roehrs, T. A., Vitaliano, P. P., Linnoila, M., & Weitzman, E. D. (1980). Effect of alcohol on sleep and nighttime plasma growth hormone and cortisol concentrations. The Journal of Clinical Endocrinology & Metabolism, 51(4), 759-764.
- St-Onge, M. P., Roberts, A., Shechter, A., & Choudhury, A. R. (2016). Fiber and saturated fat are associated with sleep arousals and slow wave sleep. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine, 12(1), 19.
- Stickgold, R and Walker, M P. (2007). "Sleep-dependent memory consolidation and reconsolidation." Sleep Med, 8: 331–343.
- Wilson, S. J., Nutt, D. J., Alford, C., Argyropoulos, S. V., Baldwin, D. S., Bateson, A. N., ... & Gringras, P. (2010). British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders. Journal of Psychopharmacology, 24(11), 1577-1601.
- Zhdanova, I. V., Wurtman, R. J., Morabito, C., Piotrovska, V. R., & Lynch, H. J. (1996). Effects of low oral doses of melatonin, given 2–4 hours before habitual bedtime, on sleep in normal young humans. Sleep, 19(5), 423-431.