 |
| The thyroid is a real diva. You better treat her with utmost care (learn more) |
If that's you, there is need for meditation, not medication, for stress management, not pills. In fact, throwing the "inactive" precursor T4, the textbook treatment for hypothyroidism into the equation, could make things even worse, as your body is going to convert the lion's share of it to the metabolic emergency break rT3, to avoid that increasing levels of the active metabolite T3 start gnawing away on your undernourished muscle and exacerbate the chronic stress you are exposing yourself to.
Is being "euthyroid" really the same as having normal TSH levels?
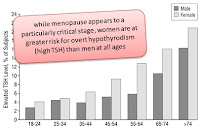 |
| Data from the The Colorado Thyroid Disease Prevalence Study indicates the risk of suboptimal thyroid function & hypothyroidism is more pronounced in women (Canaris. 2000); associations w/ certain contraception meds, pregnancy & menopause in other studies point towards estrogen / progesteron issues as confounding factors. |
While neither the average TSH levels, which were 1.92±1.06 µU/ml in the T4 and 1.87±0.89 μU/ml in the control group (P=0.91), nor the body composition (body fat: 41.4±7.4 vs 42.1±8.3%; LBM 58.6±7.4 vs 57.8±8.3%; P>0.7 for all) revealed a statistically significant inter-group difference, the resting energy expenditure of the the hypo- / after medication "euthyroid" women on levothyroxin did:
In absolute terms, the women in the T4 group had a -7% lower REE than the controls (1347±171 vs 1447±154 kcal/d; P<0.05).Click on the image to learn how to calculate (I should rather say estimate) your resting energy expenditure using different scientifically verified formulas and why it is important not to go below a certain threshold (learn more) - The -7% difference remained the same and had an even higher statistical significance (P<0.02 vs. P<0.05), when the resting energy expenditure was expressed relative to the the subjects lean body mass (28.3±2.6 vs 30.5±3.0 kcal/kg LBM die; P<0.02).
- A smaller yet still significant difference was observed when the actual resting energy expenditure was compared to the "supposed" resting energy expenditure calculated by the means of the Harris-Benedict Equation(91±7 vs 95±7%; P<0.05).

higher RER levels indicate a greater contribution of glucose, while![]()
Suggested read: Maximal Intra- & Post- Workout Fat Oxidation With Pause or 90min LISS Between 2x40min Incremental Exercise Bouts? (read more) - lower RER levels indicate a greater contribution of fats
- A RER of ~1.0 would be observed in healthy individuals, only, when they are engaging in highly glycolytic + brief exercise bouts like sprinting.
- Many "fat burners" work in part by decreasing the RER. When you are in a caloric deficit (and only then) this is an advantage because you will spare glucose and burn fat.
- Other supplements like creatine, for example, gear your metabolism towards an increase in glucose expenditure, which can be beneficial in all sorts of activities that rely heavily on short sprints / brief muscle contraction

Aren't there better alternatives? T4+T3 or dessicated thyroid?
In a way it is funny - or should I say tragic(?) - that this is the first study in years that bothers with the metabolic and often psychological downsides of T4 only regimen in a way that goes beyond the analysis of TSH levels. After all, the Internet and the waiting rooms of medical practitioners all over the world are full of (mostly female) patients complaining about the non-existent benefits and / or side effects of levothyroxin, only, therapies.
It should be obvious that some of those patients may belong to the initially referred to group of people who suffer from self-induced hypothyrodism in response to undereating and/or overtraining, while others may have confounding, often undetected pathologies that are responsible for their compromised metabolism, their inability to lose weight, their sluggishness, brain fog etc.
 |
| Suggested read: "Dietary Thyroid Treatment: Beef, Green Vegetables, Full-Fat Milk & Butter Normalize TSH in Subclinical Hypothyroidism " (read more) |
Interestingly, the patients had significantly lower rT3 levels, higher total T3 levels, lower otal and free T4 levels and that in the presence of higher, but normal TSH levels (inter-group difference p=0.032) during the DTR part of the 2x16 week cross-over trial. A health hazard, as it is often argued that it would be the result of depressed TSH levels is thus a weak argument against using an alternative treatment strategy, of which I would highly suspect that it could resolve part of the metabolic dysadvantages arising in the context of T4 monotherapy and which was preffered by 34 of the patients in the Hoang study.
Bottom line: Whether using T4 + T3 or natural dessicated thyroid as the treatment method of choice is necessary or the best strategy for everyone is something that remains to be seen. Something that stands out of question, though, is that the stubborn adherence to the textbook standards, the blind reliance on TSH tests and the ignorance doctors display towards the complaints of their patients is not going to solve an increasingly prevalent problem (+3% increase in congenital hypothyrodism per year in the US, esp. in white and hispanic newborns; cf. Hintnon. 2010)
References
- Canaris GJ, Manowitz NR, Mayor G, Ridgway E. The Colorado Thyroid Disease Prevalence Study. Arch Intern Med. 2000;160(4):526-534.
- Hinton CF, Harris KB, Borgfeld L, Drummond-Borg M, Eaton R, Lorey F, Therrell BL, Wallace J, Pass KA. Trends in incidence rates of congenital hypothyroidism related to select demographic factors: data from the United States, California, Massachusetts, New York, and Texas. Pediatrics. 2010 May;125 Suppl 2:S37-47.
- Hoang TD, Olsen CH, Mai VQ, Clyde PW, Shakir MK. Desiccated Thyroid Extract Compared With Levothyroxine in the Treatment of Hypothyroidism: A Randomized, Double-Blind, Crossover Study. J Clin Endocrinol Metab. 2013 Mar 28.
- Martucci F, Manzoni G, Lattuada G, Perseghin G. Overweight/obese women with primary acquired hypothyroidism in appropriate levothyroxine replacement therapy are characterized by impaired whole body energy metabolism. Endocrine Abstracts (2013) 32 P1004 | DOI:10.1530/endoabs.32.P1004 Share on facebook Share on twitter Share on digg Share on stumbleupon Share on delicious Share on linkedin | Share on email Share on print