 |
| If I know anything for sure, it is that the reason your midsection does not look like this, but rather like the one of Melissa McCarthy is not a result of the fact that your diet contains 24% instead of 48% fat. |
"Still outrageous, almost blaspheme!",...
... well, so were the results: There were no differences in body weight or body fat loss and as Klempel, Kroeger, Norkeviciute et al. point out "improvements in FMD [brachial artery flow mediated dilation] with ADF [alternate day fasting] may only occur with LF diets and not with HF diets" (Klempel. 2013). Or put simply - as a really obese individual, you would not really have to worry about your carb/fat ratio, if getting lean was all you were concerned about. If you want to improve your heart health, though, it appears prudent to follow a relatively low fat intake - keep in mind 25% is still more than enough to get all the fat you need for your endocrine system to keep functioning.
"Gimme the details on the study protocol!"
So, now that you've got the basic message, let's take a look at how these results actually came about: The subjects had been recruited from the Chicago area based on the following inclusion criteria: Female, age 25–65 years, body mass index between 30 and 39.9 kg m², stable weight for at least three month before the intervention, nondiabetic (this does not mean they were not insulin resistant, but it means their pancreas was not already damaged), no history of cardiovascular disease, sedentary or lightly active for at least 3 months before the beginning of the study, non-smoker, and not taking weight loss, lipid-lowering, or glucose-lowering medications. There were N = 17 an N = 18 subjects in the high and low fat groups respectively (randomized) and the total duration of the study was 8 weeks.
as mentioned before, all food was provided throughout the 10-week trial to all subjects; the diets were provided as a 3-day rotating menu consisting of typical American foods; participants were requested to eat only the foods provided and to bring back any leftover foods to be weighed and recordedAs usual, there are arguments (though not from fasting studies) on both sides of the divide; studies where people are only given lose instructions and no foods, do yet often produce very questionable results (learn more). - moreover, subjects were instructed to keep track of all food items consumed using a ‘Food checklist’, and to report any extra food item consumed using an ‘Extra food log’. If the log indicated that the subject ate extra food items (totaling 450 kcal) on a feed or fast day, that day was labeled as‘not adherent’.
- hunger, satisfaction and fullness were assessed using a questionnaire with a validated visual analog scale on each fast day; the form was completed in the evening, approximately 5 min before going to bed
- participants had to wear a pedometer each day throughout the 10-week trial, to record the free-living physical activity
- during the active weight loss pahse (weeks 3-10) subjects consumed 25% of their energy needs on the fast day (24-h period) and 125% of their energy needs on the feed day (24-h period)
- feed/ fast days began at midnight each day
- fast day meals were consumed between 12pm and 2pm
the same macronutrient composition was used during the weight loss and weight maintenance periods for each group, with...![]()
Most formulas that are used to calculate your energetic requirements are about as "accurate" as the reading from the globe in Anelina,... ah Lara's hand (learn why) - ADF-HF (45% fat, 40% carbohydrate and 15% protein),
- ADF-LF (25% fat, 60% carbohydrate and 15% protein)
- the fats in the diets consisted of
- ADF-HF (14% saturated fat, 20% monouns. fat, 11% polyuns. fat and 0% trans fat) and
- ADFLF (6% saturated fat, 13% monouns. fat, 6% polyuns. fat and, 0% trans fat)
- the energy requirements were calculated at the beginning of the study and at the beginning of the weight loss intervention using the Mifflin–St Jeor equation, using an "activity factor" of 1.2 (=sedentary; learn more about the equation)


"Ok, that's enough, what about the results"
Wow... now, that you know all the important and less important details about the methods, it's about time to eventually look at the actual outcomes of the study:
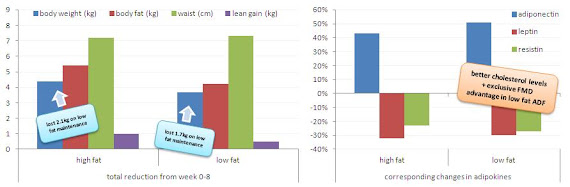 |
| Figure 1: Changes in body composition (left) and adipokine levels (right) from week 0-8 (Klempel. 2013) |
Low fat and satiety, how does this go together?
What is quite astonishing - and this goes against everything you'll hear on the Internet about the downsides of "low fat" and the benefits of "high fat diets" - is that the subjects in the low fat group, were slightly lesshungry (25 vs. 24), experienced a significantly larger increase in satifsaction (+26 vs. +1) and fullness (+20 vs. -17) and did not decrease their daily activity level to the same extent the high fat dieters did (-157 vs. -644).
Looking at the absolute levels, not the differences from baseline, the image is yet less clear. In absolute terms, the satisfaction and fullness levels, of which the scientists point out that it "started out low in the LF group, but gradually increased over 10 weeks" (Klempel. 2013).
Still, it were the participants in the low fat group who saw greater improvements in adiponectin (51±7% vs. 43±7%), a less pronounced drop in leptin (30±3% vs. 32±5%) and a minimally greater improvement in resistin (27±4% vs 23±5%; cf. figure 1) levels, none of which was found to correlate with fat mass loss and can thus expected to be diet and not fat loss specific. Furthermore, it is, as the scientists point out, well possible that it is at least partly due to these changes in adipokine expression that the low fat group saw improvements, the high fat group further deterioration in brachial artery flow mediated dilation:
As mentioned before, the other differences are actually not worth discussing and if it was not for the statistically significant improvement in the flow-mediated dilation of the brachial-artery (+2.1%), which was absent in the high fat group (-1.8% reduction in FMD, you would be hard pressed to find arguments in favor of any of the diets.Insulin is a natural NO booster: You may remember having read about it on the SuppVersity Facebook wall. Insulin has a direct effect on the NO induced widening of the arteries - as long as the cells in the arterial wall, are not already insulin resistant, that is (cf. Rajapakse. 2013). Since intermittent / alternate day fasting will help restore this insulin sensitivity, the increase in FMD could well be "insulin-dependent", as well.The role that leptin and resistin have in mediating FMD most likely involves changes in the production of NO. More specifically, leptin and resistin blunt the production of NO, which likely occurs through the stimulation of reactive oxygen species that scavenge NO and impair endothelial NO synthase function. As concentrations of these adipokines were reduced in the present trial, we would assume that there would be less leptin and resistin in the circulation to inhibit NO. This would lead to a higher production of NO, resulting in an enhancement in endothelium-dependent vasodilation. The reason why these decreases in leptin and resistin did not contribute to increases in FMD is unclear. However, it is possible that greater decreases in leptin (450%) would be necessary to improve FMD." (Klempel. 2013)
 |
| The evidence for or against low vs. high fat diets is far from being conclusive. I guess that's also why the "war" between the proponents of one or the other way of eating is fought with with no holds barred. There is still much to be learned and many results, such as the non-fattening effects of low fat diets on a caloric surplus go against the unique and all-across the board, one size fits it all benefits of low carbing (learn more) |
That being said, it is not warranted to draw any reliable conclusions wrt to a "lean gains" type of intermittent fasting in athletic individuals based on the study at hand. In my humble opinion, there is yet no good reason that would speak in favor of going low carb either. This is particularly true if you are adding a reasonable workout routine that goes beyond doing a one-rep max effort per day to exponentiation the results of the diet. In that case, you are better off providing your muscles and liver with glucose directly than having the latter produce it from protein (first) and fat (second), which is what will necessarily happen unless you are eating so little protein that you actually make it into full ketosis.
References:
- Klempel MC, Kroeger CM, Norkeviciute E, Goslawski M, Phillips SA, Varady KA. Benefit of a low-fat over high-fat diet on vascular health during alternate day fasting. Nutr Diabetes. 2013 May 27;3:e71.
- Rajapakse NW, Chong AL, Zhang WZ, Kaye DM. Insulin-mediated activation of the L-arginine nitric oxide pathway in man, and its impairment in diabetes. PLoS One. 2013 May 2;8(5):e61840.