 |
| A lack of libido appears - if at all - treatable w/ DHEA only in peri-menopausal women (Maggi. 2013; Pucchino. 2013); there are however a lot of other things DHEA can do for you. |
On a related note: Downloading the podcast is also well worth it, because you get Chris Masterjohn's interview on vitamin D as a "free goodie". Well worth it, I promise (download the podcast).
Let's not waste time, but get straight to the point
As you have heard DHEA is the most abundant steroid hormone in your body, it is produced in the mainly in the adrenal gland (~31mg in men and 18mg in women). In women specifically, DHEA is also the main precursor to androgens (testosterone, DHT & metabolites). For both men and women DHEA and DHEA-S the most abundant, sulfur-bound stable transport form of DHEA. It acts as a neurosteroid the age-induced decline of which has long been implicated as one, if not the main hormonal underpinnings of the cognitive decline we experience as we age.
 |
| Figure 1: Age-induced decline in DHEA, effects of oral contraceptice use, hormonal cascade that leads to the formation of DHEA (enzymes to the side) and overview of reasons for DHEA decline. |
Fitness is rewarded: Did you know that men who exercise regularly have 2x higher DHEA-S levels than sedentary slobs? they also have 41% lower body fat %-ages (Tissandier. 2001) - coincidence? Probably not! Being fat lowers DHEA and low DHEA increases fat gain (Pritchard. 1998). The beneficial effects of DHEA on body comp, on the other hand, are mediated by the modulation of the effects of cortisol (listen to the show) and direct lipolytic effects on subcutaneous (women) and visceral (men) fat (Hernández-Morante. 2008; more evidence).
Specifically with respect to the cognitive effects, or rather their absence in corresponding trials, it may yet well be that our problem is administration specific and/or of pharmacokinetic nature and thus a mere result of the fact that you cannot replace the endogenously produced DHEA in the central nervous system (which is next to the gonads #2 of the non-adrenal tissues that is capable of synthesizing DHEA from pregnenolone; Dong. 2012). The short-lived pronociceptive (=pain reducing) effects (<150min) of oral DHEA supplementation at 10mg/kg in rodents would furthermore suggest that we are not so much suffering from low systemic levels as we are from our bodies inability to regulate DHEA levels on demand (Gąsińska. 2012).Apropos regulating DHEA levels "on demand"
Actually DHEA is supposed to increase in response to stress. When stress is becoming "normal", however, the stress-induced DHEA release becomes blunted (Lennartsson. 2013). This process is actually characteristic of the early stages of "adrenal fatique" - I deliberately use the term in quotation marks, because there is no "fatigue" involved here, it's a "simple" deregulation of the up and down that should be characteristic of our stress natural and health response; see "Science Round-Up Seconds: All About Cortisol, Fat Loss, Body Composition and the Efficacy & Safety of 7-Keto & Co" | read more.
And while it may make some sense to supplement with DHEA in the early stages of "adrenal fatigue" (high cortisol, minimally decreased DHEA) its "anti-cortisol" effects are going to do more harm than good, once the initially high cortisol levels are breaking away, and dropping from high to rock bottom. In these latter stages of adrenal fatigue DHEA only treatments could actually make you believe that life sucks even more than it does already.
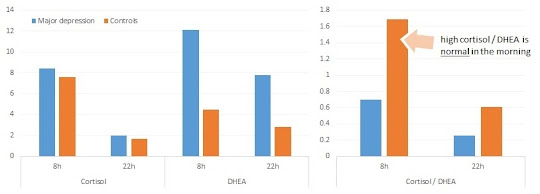 |
| Figure 2: Elevetated DHEA levels in the AM and PM and a low DHEA / cortisol ratio in the AM (8h) are characteristic of patients with major depression (Assies. 2004) |
"DHEA-S was significantly elevated, in conjunction with normal cortisol levels. Based on DHEA-S at 22:00 h only, 77% of the subjects were correctly classified in a discriminant analysis as depressed or control. When simultaneously entered in a multiple regression analysis, DHEA-S (morning and evening) and cortisol (evening only) predicted symptom severity in depressed patients. These preliminary results suggest that DHEA-S may be a more sensitive indicator of depression and symptom severity than cortisol in medicated but still clinically depressed patients." (Assies. 2004)Surprised? You shouldn't be. At least as a regular here at the SuppVersity you should by now be aware that more of a good thing is not necessarily better.
Too much of a good thing is probably also the reason for most side effects
I actually went into pretty much detail on the connection between dosing schemes and ranges, on the one hand, and potential side effects, on the other hand during the live show, already. I will therefore stick to a reminder here: The more DHEA you take, and the higher the individual dosages, the greater the hard-to-predict conversion to androgens and estrogens.
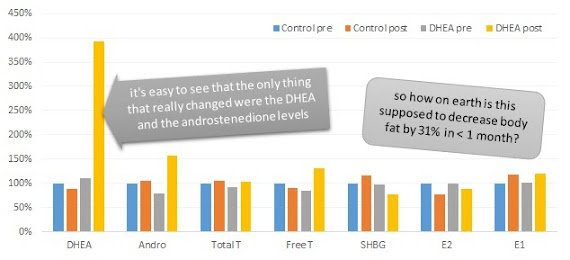 |
| Figure 3: These hormone levels (expressed relative to placebo control at baseline) do not look exactly as if they would be able to induce a -31% reduction in body fat within one month. Plus: They do by no means look like the results of 1,600mg of DHEA per day - that would be ~53x more than your body produces on a daily basis (data adapted from Nestler. 1988) |
"The men then took orally, in a double blind fashion, capsules containing either placebo or 400mg(138.7mmol) DHEA four times daily [total daily DHEA dose, 1600mg or 28days]." (Nestler. 1988)
 |
| The data in the study at hand is even less credible, if we look at the results of a more recent study which showed age- dependent increases of 100-300% in testosterone, when young(er), middle aged and older men took 50mg of DHEA the night before they undertook a HIIT regimen (learn more)... but hey, maybe the guys trained once during the 30 day study period and hat a 3000% T-boost |
- whether these results are accurate or simply the result of faulty measurements
- if more than 10% of the ingested DHEA actually was absorbed
High estrogen is not a regular side effect
No, no and no. Look at the data from the Nestler study. 1,600mg per day and NO (=ZERO) change in estrogen. This is however not the norm - the norm is a proportional increase in estrogen and testosterone which tends to leave healthy men with a higher testosterone to estrogen ratio than before. Examples? Here you go:
 |
| Figure 4: Effects of 50mg DHEA for 36 months in 70yr old men (left) and 100mg of DHEA for 6 months in men and women (Müller. 2006; Morales. 1998) |
The Morales study should by the way remind us of one of the most important functions of DHEA in women - it's the main precursor to male sex hormones (here testosterone Figure 4, right-top and DHT Figure 4, right-bottom); as discussed further down, DHEA can thus in fact be used as a "HRT"-like treatment in women, but not in men.
So who can benefit?
Actually the previously mentioned sex difference segues nicely into my here's who benefits list, Carl and I did not really have the time to cover, yesterday... so let's see:
people with low (age-corrected) DHEA levels - in this case DHEA is like any other hormone replacement therapy and should be monitored by a medical professional of whom you should make sure that he controls for confounding factors that would point towards confounding and causal factors![]()
DHEA increases Testosterone & Blunts Muscle Damage (read more) - people in their late 40s or later - as discussed in the show, the changes in hormonal levels, body comp and quality of life questionnaires may not be significant, but if you compare them to the control groups there is usually a benefical trend (gaining muscle and losing fat is better than the other way around, even if its only in the 500g range; cf. Müller. 2006; also discussed in the live show); still in view of the fact that you really don't know what you will get - get tested (must: DHEA-S, testosterone, DHT, estrogen (E2); optional: SHBG, free testosterone, E1, insulin, cholesterol panel, PSA (addition as per Daria's suggestion) - the latter two may in fact improve, by the way) after 1-2 months and every 6 months thereafter
men and women with low androgens - though (esp. for men) "real HRT" is probably the better way to go, you can try what I outlined for 40+ agers to bump up your androgens, as well![]()
DHEA blunts fat deposition more effectively than testosterone; for both the effects are mediated via PPAR-gamma (read more) - women in early menopause - benefits have been observed for both the Kupperman score (index to quantify menopause symptoms) and vasomotor symptoms of menopause (Stomati. 2000).
Some authors even consider it an adequate hormone replacement alternative for women (both studies used "only" 50mg/day!):
another pro-argument is certainly the increase bone mineral density, which is and will probably always remain one of the major issues in menopause.
"Administration of DHEA significantly affects several endocrine parameters in early and late postmenopausal women independently from body mass index. Our data support the hypothesis that DHEA treatment acts similarly to estrogen-progestin replacement therapy on the GHRH-GH-IGF-1 axis. This suggests that DHEA is more than a more than a simple "diet supplement" or "antiaging product"; rather it should be considered an effective hormonal replacement treatment." (Genazzani. 2001)![]()
Suggested read: "Carnitine as Repartitioning Agent? IGF-1, p-AKT & mTOR Up, Catabolic Proteins Down + 7% Improvement in Lean- to Total Mass Ratio" | read more - Other things worth mentioning: Actually I have a couple of pages of additional notes, but I guess these are the most interesting points → DHEA increases intramuscular DHT, which is associated with increased insulin sensitivity (Sato. 2011) → DHEA improves both GLUT-4 and Akt (could also increase protein synthesis) in diabetic rodents (Sato. 2009) → DHEA improves the levels of the master anti-oxidant GSH in aging (or sick) livers (Jacob. 2011) → DHEA slows the development of type II diabetes (Byrne. 2001; rodent model) → Salivary cortisol and DHEA-S concentrations reflect the activity of the HPA axis (Ghiciuc. 2011) → DHEA opposes the immune suppressive effects of cortisol (Chen. 2004) → DHEA has thermogenic effects (Lardy. 1995) → DHEA is on the WADA list of prohibited substances, but doping researchers say its effect / side effect profile is not worth it anyway (Hahner. 2010) → DHEA has anti-breast cancer effect in rodent model of developing mammary cancer (via conversion to androgens; Labrie. 2001)men and women with hyperthyroidism - the increased thyroid activity "burns" through all adrenal hormones, so that backup (of both DHEA and cortisol) can become necessary (Agbaht. 2013)
- patients on glucocorticoids (e.g. for inflammatory or immune diseases) - cortisol and synthetic glucocorticoids suppress DHEA production - it's thus logical that backfilling the missing hormones can help
- people on severe chronic stress - the military, for example has conducted a handful of interesting studies; two of the most recent studies were conducted by Taylor et al. (2012) and Taylor (2013) - the researchers report neuroprotective and anabolic effects with 50mg/day (classroom phase) and 75mg/day (training in the field), respectively
- people using non-aromatizing steroids - DHEA can provide a precursor for a baseline estrogen level even on suppressive non-aromatizing drugs (listen to the show for more details)
- patients suffering from lupus erythematosus ["syndrome like" = very unspecific autoimmune disease usually with sever joint pain and arthritis, ca. 5 mio people world-wide suffer; every year 100,000 new cases in the US / constantly increasing (Buvat. 2003); honestly I suspect this leaves more cortisol to get the inflammation under control, but hey what do I know; usually women, often African American or latino] proven benefit from 200mg/day
- women with diminished ovarian reserve - while the latest review says the evidence was not there, I consider the results of a study by Gleicher (2009), alone, worth giving it a try: The researchers observed a restoration of the rate of miscarriages to normal levels in the 73 cases they evaluated – that’s a reduction of -51% risk of having a miscarriage and direct effect on the occurrence of genetic disorders like "Trisomy 21" [= down syndrome] in women with diminished ovarian reserve (Gleicher. 2010) - still: don't even think about messing with your hormones, when you are healthy and wand to become pregnant!



 |
| Suggested read for those who cannot get enough of DHEA stories: "Less Than 15mg of DHEA Exert Identical Beneficial Effects on Insulin Sensitivity as 1h of Cardio 5x Per Week. Both Effects Mediated Via Increases in Intra-Muscular DHT" | read more, expect similar, but not 1:1 identical results in humans |
Whether the latter will or won't have beneficial effects will vary from person to person and makes testing all the more important. If you remember that and the fact that the fairy tales on the bulletin boards all over the Internet don't provide an adequate picture of what works, what sucks and what you side effects will or won't occur (listen to the podcast for additional details), I'd say you know plenty about DHEA... and if you disagree, just check out what I previously wrote about DHEA, here.
References:
- Agbaht K, Gullu S. Adrenocortical reserves in hyperthyroidism. Endocrine. 2013 Mar 27.
- Assies J, Visser I, Nicolson NA, Eggelte TA, Wekking EM, Huyser J, Lieverse R, Schene AH. Elevated salivary dehydroepiandrosterone-sulfate but normal cortisol levels in medicated depressed patients: preliminary findings. Psychiatry Res. 2004 Sep 30;128(2):117-22.
- Buvat J. Androgen therapy with dehydroepiandrosterone. World J Urol. 2003 Nov;21(5):346-55. Epub 2003 Oct 10. Review.
- Byrne JJ, Bradlow HL. DHEA-PC slows the progression of type 2 diabetes (non-insulin-dependent diabetes mellitus) in the ZDF/Gmi-fa/fa rat. Diabetes Technol Ther. 2001 Summer;3(2):211-9.
- Chatzittofis A, Nordström P, Hellström C, Arver S, Asberg M, Jokinen J. CSF 5-HIAA, cortisol and DHEAS levels in suicide attempters. Eur Neuropsychopharmacol. 2013 Feb 28.
- Chen CC, Parker CR Jr. Adrenal androgens and the immune system. Semin Reprod Med. 2004 Nov;22(4):369-77.
- Dong Y, Zheng P. Dehydroepiandrosterone sulphate: action and mechanism in the brain. J Neuroendocrinol. 2012 Jan;24(1):215-24.
- Gąsińska E, Bujalska-Zadrożny M, Sar M, Makulska-Nowak H. Influence of acute and subchronic oral administration of dehydroepiandrosterone (DHEA) on nociceptive threshold in rats. Pharmacol Rep. 2012 Jul;64(4):965-9.
- Genazzani AD, Stomati M, Strucchi C, Puccetti S, Luisi S, Genazzani AR. Oral dehydroepiandrosterone supplementation modulates spontaneous and growth hormone-releasing hormone-induced growth hormone and insulin-like growth factor-1 secretion in early and late postmenopausal women. Fertil Steril. 2001 Aug;76(2):241-8.
- Ghiciuc CM, Cozma-Dima CL, Pasquali V, Renzi P, Simeoni S, Lupusoru CE, Patacchioli FR. Awakening responses and diurnal fluctuations of salivary cortisol, DHEA-S and α-amylase in healthy male subjects. Neuro Endocrinol Lett. 2011;32(4):475-80.
- Gleicher N, Ryan E, Weghofer A, Blanco-Mejia S, Barad DH. Miscarriage rates after dehydroepiandrosterone (DHEA) supplementation in women with diminished ovarian reserve: a case control study. Reprod Biol Endocrinol. 2009 Oct 7;7:108.
- Gleicher N, Weghofer A, Barad DH. Dehydroepiandrosterone (DHEA) reduces embryo aneuploidy: direct evidence from preimplantation genetic screening (PGS). Reprod Biol Endocrinol. 2010 Nov 10;8:140.
- Hahner S, Allolio B. Dehydroepiandrosterone to enhance physical performance: myth and reality. Endocrinol Metab Clin North Am. 2010 Mar;39(1):127-39, x.
- Hildreth KL, Gozansky WS, Jankowski CM, Grigsby J, Wolfe P, Kohrt WM. Association of serum dehydroepiandrosterone sulfate and cognition in older adults: sex steroid, inflammatory, and metabolic mechanisms. Neuropsychology. 2013 May;27(3):356-63.
- Jacob MH, Janner Dda R, Araújo AS, Jahn MP, Kucharski LC, Moraes TB, Dutra Filho CS, Ribeiro MF, Belló-Klein A. Dehydroepiandrosterone improves hepatic antioxidant reserve and stimulates Akt signaling in young and old rats. J Steroid Biochem Mol Biol. 2011 Nov; 127(3-5):331-6.
- Labrie F, Luu-The V, Labrie C, Simard J. DHEA and its transformation into androgens and estrogens in peripheral target tissues: intracrinology. Front Neuroendocrinol. 2001 Jul;22(3):185-212. Review.
- Lardy H, Kneer N, Bellei M, Bobyleva V. Induction of thermogenic enzymes by DHEA and its metabolites. Ann N Y Acad Sci. 1995 Dec 29;774:171-9.
- Lennartsson AK, Theorell T, Kushnir MM, Bergquist J, Jonsdottir IH. Perceived stress at work is associated with attenuated DHEA-S response during acute psychosocial stress. Psychoneuroendocrinology. 2013 Sep;38(9):1650-7.
- Maggi M, Buvat J, Corona G, Guay A, Torres LO. Hormonal causes of male sexual dysfunctions and their management (hyperprolactinemia, thyroid disorders, GH disorders, and DHEA). J Sex Med. 2013 Mar;10(3):661-77.
- Morales AJ, Haubrich RH, Hwang JY, Asakura H, Yen SS. The effect of six months treatment with a 100 mg daily dose of dehydroepiandrosterone (DHEA) on circulating sex steroids, body composition and muscle strength in age-advanced men and women. Clin Endocrinol (Oxf). 1998 Oct;49(4):421-32.
- Muller M, van den Beld AW, van der Schouw YT, Grobbee DE, Lamberts SW. Effects of dehydroepiandrosterone and atamestane supplementation on frailty in elderly men. J Clin Endocrinol Metab. 2006 Oct;91(10):3988-91.
- Nestler JE, Barlascini CO, Clore JN, Blackard WG. Dehydroepiandrosterone reduces serum low density lipoprotein levels and body fat but does not alter insulin sensitivity in normal men. J Clin Endocrinol Metab. 1988 Jan;66(1):57-61.
- Pluchino N, Carmignani A, Cubeddu A, Santoro A, Cela V, Alcalà TE. Androgen therapy in women: for whom and when. Arch Gynecol Obstet. 2013 Aug 3.
- Pritchard J, Després JP, Gagnon J, Tchernof A, Nadeau A, Tremblay A, Bouchard C. Plasma adrenal, gonadal, and conjugated steroids before and after long-term overfeeding in identical twins. J Clin Endocrinol Metab. 1998 Sep;83(9):3277-84.
- Sato K, Iemitsu M, Aizawa K, Ajisaka R. DHEA improves impaired activation of Akt and PKC zeta/lambda-GLUT4 pathway in skeletal muscle and improves hyperglycaemia in streptozotocin-induced diabetes rats. Acta Physiol (Oxf). 2009 Nov;197(3):217-25.
- Sato K, Iemitsu M, Aizawa K, Mesaki N, Fujita S. Increased muscular dehydroepiandrosterone levels are associated with improved hyperglycemia in obese rats. Am J Physiol Endocrinol Metab. 2011 Aug;301(2):E274-80.
- Stomati M, Monteleone P, Casarosa E, Quirici B, Puccetti S, Bernardi F, Genazzani AD, Rovati L, Luisi M, Genazzani AR. Six-month oral dehydroepiandrosterone supplementation in early and late postmenopause. Gynecol Endocrinol. 2000 Oct;14(5):342-63.
- Taylor MK, Padilla GA, Stanfill KE, Markham AE, Khosravi JY, Ward MD, Koehler MM. Effects of dehydroepiandrosterone supplementation during stressful military training: a randomized, controlled, double-blind field study. Stress. 2012 Jan;15(1):85-96.
- Taylor MK. Dehydroepiandrosterone and dehydroepiandrosterone sulfate: anabolic, neuroprotective, and neuroexcitatory properties in military men. Mil Med. 2013 Jan;178(1):100-6.
- Tissandier O, Péres G, Fiet J, Piette F. Testosterone, dehydroepiandrosterone, insulin-like growth factor 1, and insulin in sedentary and physically trained aged men. Eur J Appl Physiol. 2001 Jul;85(1-2):177-84.