 |
| In contrast to the message "trans fats = bad". The information that cookies and bakery, not cooking oil, margarine, chips & co are the main trans fat offenders in our diet has reached only a very small group of people. |
The question I would like you to remember, when you read more about the most recent strudy from the Preventive Cardiology Program at the Columbia University Medical Center/New York-Presbyterian Hospital in 2013 is:
Do those 0.5g/serving the FDA is turning a blind eye on matter?
Within the past decades, the ill health effects of transfats have been addressed by countless studies. The study at hand, however, is the first one to directly assess and quantify the influence of transfats on LDL particle number (LDL-P = particle number, not LDL-C = LDL content!).
"Studies have suggested that increased LDL-P leads to progression of CVD and that the predictive value of LDL-P for future CVD events is equal to or greater than more traditional lipid measurements such as LDL-C." (Garshik. 2013)That alone is a huge plus, but guess what: M. Garshick, H. Mochari-Greenberger and L. Mosca have been working with real patients - no rodents.. ah pardon, strings attached ;-)
This is not just another rodent study
Having the advantage of actually working in a hospital, not a sterile lab setting, the researchers picked participants from the Family Intervention Trial for Heart Health (FIT Heart), a National Heart Lung and Blood Institute (NHLBI) sponsored randomized controlled clinical trial that enrolled 501 family members of patients who were admitted to the cardiovascular service of the New York Presbyterian/Columbia University Medical Center, as their subjects. In the course of a previous study, the subjects had been assigned to two different groups:
An intervention group,the members of which were invormed about the CVD risk factor screening results and education about diet and physicalactivity to prevent CVD, with regular contact and feedback by a health educator for up to 1-year, and![]()
Table 1: Subject characteristics at baseline (Garshik. 2013) - A control group, that did not receive the information about their own CVD risk factor and was not part of the organized education program that did obviously include the advise to reduce your trans-fat intake as much as possible

Is it bad, if you get 2.5% of your daily energy intake from trans-fats?
When all was said and done, M. Garshick, H. Mochari-Greenberger and L. Mosca ended up with a "participant pool" the characteristics of which you I've summarized in Table 1. If you stop gazing at Table 1 and take a look that the data in Table 2, you will see that the average subject consumed approximately 2.5% of his or her daily energy intake from trans-fats.
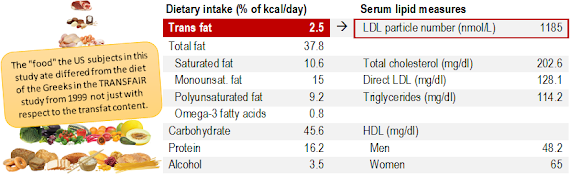 |
| Table 2: Dietary intake (% of kcal/day) and corresponding serum lipid measures in the subjects of the Garshick study. |
The Greeks on the other hand, live up to their reputation as the fathers of the often-hailed Mediterranean Diet: With a mean trans-fat intake of 0.5% and 0.8% in men and women, respectively, they are compliantwith the recommended maximal daily allowance (RDA) of 2.2g trans-fats per day (this statement is based on the assumption that their average caloric intake was 2,000kcal).
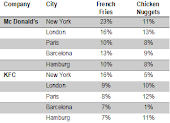
You don't have to move to Greece though, to reduce your personal trans-fat intake even further. It is, after all, another flawed urban nutrition myth that you could produce trans-fatty acids in your kitchen by heating whatever type of oil / fat you use to cook (if you never change the oil you use to fry at very high temperatures, things look different, though). Industrially produced junk... ah, pardon "food" - specifically cakes, cookies, etc. - is thus your most if not only significant source of dietary trans-fats. Eliminate those and you are good to go.
Remember: Higher baseline intake = greater relative effect size!
 |
| Figure 1: Linear associations between baseline dietary composition and LDL particle number (top) and between change in dietary trans-fat intake and LDL particle number in the course of 1-year (bottom); data based on Garshik, 2013. |
If we discard the effect size and focus on the general trend, the results of the Garshik study are still highly relevant for all of us; and what's more, most of us will have friends or relatives with similar transfat intakes, a low activity level, a low MUFA and omega-3 intake and way too little protein in their diets - and as Figure 1 can tell you, MUFAs, n-3s, protein and obviously exercise / physical activity are all factors that have been found to be associated with low(er) LDL particle counts and a correspondingly increased risk of arteriosclerosis and heart disease in the Garshik study (see Rosenson. 2002 & 2010; Prado. 2011 for the link between LDL-P and heart health).
 |
| Eggs are trans-fat free and heart-healthy | learn why. |
If we assume that there is a linear relationship between LDL-P and trans-fat intake (obviously this is a gross simplification) and make a rough and scientifically highly questionable estimate of the consequences, we will find that those unlabeled 0.5g of transfats could boost your LDL levels from the first into the third tertile of LDL-P values in the Prado study (+by 675nmol/L).... that this would also mean that a daily dose of only 0.5g of hidden trans-fats could triple your likelihood of arteriosclerotic plaque should be obvious, right?
References:
- Cromwell WC, Otvos JD, Keyes MJ, Pencina MJ, Sullivan L, Vasan RS, et al. LDL particle number and risk of future cardiovascular disease in the Framingham offspring study-implications for LDL management. J Clin Lipidol 2007 Dec;1(6):583-92.
- Cromwell WC, Otvos JD. Low-density lipoprotein particle number and risk for cardiovascular disease. Curr Atheroscler. Rep 2004 Sep;6(5):381-7.
- Garshick M, Mochari-Greenberger H, Mosca L. Reduction in dietary trans fat intake is associated with decreased LDL particle number in a primary prevention population. Nutr Metab Cardiovasc Dis. 2013 Oct 4.
- Hulshof KF, van Erp-Baart MA, Anttolainen M, Becker W, Church SM, Couet C, Hermann-Kunz E, Kesteloot H, Leth T, Martins I, Moreiras O, Moschandreas J, Pizzoferrato L, Rimestad AH, Thorgeirsdottir H, van Amelsvoort JM, Aro A, Kafatos AG, Lanzmann-Petithory D, van Poppel G. Intake of fatty acids in western Europe with emphasis on trans fatty acids: the TRANSFAIR Study. Eur J Clin Nutr. 1999 Feb;53(2):143-57. Review.
- Mora S. Advanced lipoprotein testing and subfractionation are not (yet) ready for routine clinical use. Circulation 2009 May 5; 119(17):2396-404.
- Mosca L, Mochari H, Liao M, Christian AH, Edelman DJ, Aggarwal B, et al. A novel family-based intervention trial to improve heart health: FIT Heart: results of a randomized
controlled trial. Circ Cardiovasc Qual Outcomes 2008 Nov; 1(2):98-106. - Prado KB, Shugg S, Backstrand JR. Low-density lipoprotein particle number predicts coronary artery calcification in asymptomatic adults at intermediate risk of cardiovascular disease. J Clin Lipidol 2011 SepeOct;5(5):408-13.
- Rosenson RS, Otvos JD, Freedman DS. Relations of lipoprotein subclass levels and low-density lipoprotein size to progression of coronary artery disease in the Pravastatin Limitation of Atherosclerosis in the Coronary Arteries (PLAC-I) trial. Am J Cardiol 2002 Jul 15;90(2):89.94.
- Rosenson RS, Davidson MH, Pourfarzib R. Underappreciated opportunities for low-density lipoprotein management in patients with cardiometabolic residual risk. Atherosclerosis 2010 Nov; 213(1):1-7.
- Stender S, Dyerberg J, Astrup A. High levels of industrially produced trans fat in popular fast foods. N Engl J Med. 2006 Apr 13;354(15):1650-2.