 |
| Both ladies are D-ficient, but will probably need profoundly different amounts of D3 to get their 25OHD back in range. |
I am honestly not yet sure what exactly we will cover today, but among the things I am still thinking about how we can squeeze them into a 1h show are...
- methylxanthines caffeine, theobromine and theophylline can bind to human DNA - what does that tell us about the purported health benefits of caffeine & co?
- caffeine prevents memory impairment - in this case in a model of sporadic Alzheimer's disease
- anti-Alzheimer's effect of CLA - plus a list of supplements that have been implicated in the prevention of Alzheimer's and other amyloid diseases such as Parkinson's, Cerebellar Ataxis, Amyotrophic lateral sclerosis and (hardly recognized as an amyloid disease) diabetes type II
- the effect of body weight on the benefits of circuit training in older women - turns out that those who need it the most, namely the obese, also see the greatest benefits
- Gum arabicum to ward off holiday weight gain - that this could actually work is at least what a recent human study would suggest
- more on vitamin E, resveratrol, soldiers don't get hurt in battle, but by geranium (DMAA), ...
Let's get to the D-news, now
The general consensus among the vitamin D advocates currently is that 2,000 IU of vitamin D3/day is the minimum you need to bring low levels of 25OHD back into the normal range. A soon-to-be-published study by Gallagher, Yalamanchili and Smith that's available ahead of print on the website of the Journal of Steroid Biochemistry and Molecular Biology does yet contradict this notion - at least for women with a body mass <25kg/m² even the meager RDA of 400IU would be enough (Gallagher. 2012). That said the concise paper actually describes the results of two, not just one experiment, with
- study 1 (ViDOS) being a one-year randomized, double-blind placebo controlled study (ViDOS – Vitamin D supplementation in Older Subjects) of increasing doses of vitamin D3 (400, 800, 1600, 2400, 3200, 4000 or 4800 IU/day vitamin D3 vs. placebo + calcium supplements to maintain calcium intake between 1,200-1,400mg/day) in 163 Caucasians, age 57–90 years; all vitamin D insufficienty, i.e. serum 25OHD ≤ 20 ng/ml (50 nmol/l), and
- study 2 (STOP IT) being a 3-year intervention study of calcitriol 0.25 mcg (the active form of vitamin D) twice daily, conjugated estrogens 0.625 mg daily, a combination of both and placebo in 488 elderly women, age 65–77 years
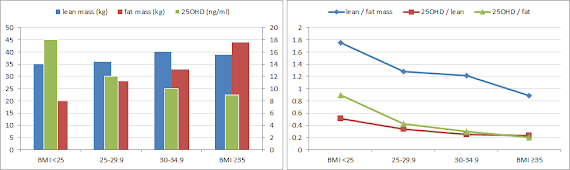 |
| Figure 1: Mean total body weight, total body lean mass, total body fat mass and serum 25OHD in different BMI subgroups of study 2 (STOPIT); right, corresponding calculated ratios (based on Gallagher. 2012). |
Being lean is a positive predictor of increases in 25OHD with supplementation
That this latent "chubbiness" of the average Westerner may be of particular significance in view of the negative / non-significant outcomes in many of the vitamin D supplementation trials, becomes self-evident, when you take a closer look at the data in figure 2, however you will have to realize that my plot which comprises above all the highly relevant relative changes (middle, marked in red) tells a different story than the original plot from the study showing only the absolute changes (left, but in form of a line graph).
 |
| Absolute, relative (compared to baseline) changes and total 25OHD levels (ng/ml) after supplementation with low, medium and high amounts of vitamin D3 in lean, normal, overweight and obese women (based on Gallagher. 2012) |
Bottom line: The data from this most recent investigation into the differential response of lean, normal, overweight and obese women to vitamin D3 supplementation shows that the absolute increases appear on BMI and that...
low dose supplementation (400 or 800IU/day) is probably only sufficient to rise and maintain adequate vitamin D levels in lean women,Always take vitamin D with fatty foods! (see "A Fat D-Ficiency") - medium dose supplementation (1,400 or 2,400IU/day) yields the most favorable outcomes in total 25OHD levels and
- high dose supplementation (3,200, 4,000 or 4,800IU/day) does not yield additional benefits in either the the normal-, overweight and obese subgroup and only marginally higher levels in the lean women.

 |
| These longissimus dorsi slices of mice on a normal and a vitamin D3 supplemented diet show that supplemental vitamin D3 can be used as a fat synthesizer and meat tenderizer in "meat-producing animals". (learn more) |
Lastly, a beneficial effect of increase / normalized vitamin D levels on lean or fat mass was (once again) not observed in any of the studies; and that despite the fact that "body fat was an independent predictor of serum PTH", which decreased in response to calcitriol supplementation in study 2 (which is actually more of an adjunct for correlative analysis and as a data source to compare the results of study 1 to). In other words, normalizing your vitamin D levels without taking appropriate measures to counter what's probably behind both, the nasty body fat and the low vitamin D level is not going to make you lean or musclar - at least as of now, it rather appears as if this was yet another instance, where we are - if anything - treating isolated symptoms instead of the root causes of the obesity epidemic.
References
- Gallagher JC, Yalamanchili V, Smith LM. The Effect Of Vitamin D Supplementation On Serum 25OHD In Thin And Obese Women. J Steroid Biochem Mol Biol. 2012 Dec 11.
- Jakobsen H, Maribo A, Bysted HM, Sommer OH. 25-Hydroxyvitamin D3 affects vitamin D status similar to vitamin D3 in pigs – but the meat produced has a lower content of vitamin D. British Journal of Nutrition. 2007; 98 908–913.
- Shephard RJ. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med. 2003 Jun;37(3):197-206; discussion 206.