 |
| Intense training sessions will always increase ALT, AST & CK. Unfortunately doctors will never learn that in med-school. |
Let's first see what we are actually talking about. Typically you went for a routine blood work and get a call from the nurse that there was something wrong with your "liver"- or "muscle-enzymes". You are summoned into the doctor's office, where your concerned doctor is already waitingat his desk looking at you as if you were a criminal and an idiot: "Do you dosteroids?"
No, creatine is not the reason your creatine kinase levels are increased?

Creatine Doubles 'Ur GainZ!

Creatine, DHT & Broscience

Creatine Better After Workout

ALA + Creatine = Max Uptake?

Creatine Blunts Fat Loss?

Build 'Ur Own Buffered Creatine
*STOP!* Agonizing about what you could possibly have done wrong is not going to help you here. This is all the more true if we take into account that tit is very likely that you did not do anything wrong at all. Against that background I'd suggest you stop panicking and start reading today's SuppVersity article, which will inform you about (1) what exactly AST, ALT and CK are, (2) why your doctor is so concerned about their elevation, and (3) how you can find out if he is rightly concerned or you are in the midst of a fitness version of Much Ado About Nothing.
What exactly are AST, ALT and CK & how do you read them (in contrast to your Dr)
On the text-book level this question is easy to answer. I guess it'd be best if we started with the proper name, of which you'll see that they already give away half of the solution to the mystically ALT, AST and CK elevations and the rarely measured but often likewise elevated lactate dehydrogenase and myoglobin levels.
 |
| Table 1: Time in h before ALT, AST, etc. (➚) exceed reference, (☆) peak, (➘) are back to normal (Petterson. 2007) |
- ALT - alanine transaminase formerly SGPT, serum glutamic-pyruvic transaminase
- AST - aspartate transaminase formerly SGOT, serum glutamic oxaloacetic transaminase
- CK - creatine kinase
- LD - lactate dehydrogenase
- Myoglobin - iron- and oxygen-binding protein
Elevated CK = Intense workout ↛ rhabdomyolysis ⇆ cardiac infarction
Did you ever notice that most lab reports list two types of creatine kinase? No? Usually they are listed as CK-MM and CK-MB and denote two out of a total seven isoforms scientists and doctors who specialize in muscular disorders are regularly testing for:
CKB ➫ brain | BB-CK![]()
Suggested Read: "Why training over the full ROM counts" | more - CKBE ➫ ectopic expression | n.a.
- CKM ➫ all muscle | MM-CK
- CK-MM ➫ mostly skeletal muscle
- CK-MB ➫ mostly heart muscle
- CKMT1A, CKMT1B ➫ ubiqu. mitochondrial CK
- CKMT2 ➫ sarcomeric mitochondrial CK

The CK-MM differntial diagnosis: Have you sustained a cardiac infarction?
I should have mentioned it before, but I believe you are smart enough not to take this article as an invitation to recklessly ignore your Dr's calls. The first thing you would want to do, when the doctor's receptionist is calling it to ask her for the exact CK-MM and CK-MB values.
Tip #1: Always insist on a print-out of all your lab values. The receptionist may say that she cannot pass confidential health information via the telephone, but neither she nor your doctor have the right to keep all or parts of your medical records from you. You paid for the lab report, so it's your property and the least your doctor can do, is handing you a copy or printout of the results. File the sheets in a folder for reference and make sure you never lose that folder.
Their ratio, i.e. the ratio of "skeletal specific" and "heart speficic" creatine kinase, can tell you whether it makes sense / is necessary to further investigate the presence of weak and not even noticeable cardiac infarction.- A follow up on your heart health is indicated, if CK-MB is elevated and higher than 5% of the total CK (CK-MM) value | example: CK-MB = 200 + CK-MM = 1000
Irrespective of all uncertainties, it is very unlikely that your heart has actually taken a beating, if you are and have always been symptom free and have a high CK-MM:CK-MB ratio. This is particularly true if you have been training in the days before the blood draw.
 |
| Figure 1: Serum creatine kinase levels (in µkat/L) of perfectly healthy young men after a single intense full-body workout (left); exercise selection (right) - all exercises were performed for 3 sets à 12 reps with 70% of the 1-RM max, the average total weight moved during a single workout was >10 metric tonnes (Petterson. 2007) |
- the creatine kinase elevations peaked 3-4 days after the workout
- the peak values vary from 'well within range' (= within the green box) to 6x above normal
Tip #2: Tell your doctor, when you've been lifting before the blood draw! If your medical practitioner does not know you and your training practices you can hardly blame him for being concerned about your health, when your creatine kinase levels are 10x-200x elevated.
It goes without saying that neither the 'low -', nor the four 'high responders' in the Petterson study had to be transferred to the emergency room for impeding kidney damage in response to full-blown rhabdomyolysis and that despite the fact that their levels were - due to their low training status - much more pronounced than those of the average athlete.If you train like an athlete you will have the creatine kinase levels of an athlete
Irrespective of the protective effects of regular exercise, even professional athletes have chronically elevated creatine kinase levels. Yet, despite the fact that a 1984 study by Jaffe et al. was by no means the first to conclude that a substantial fraction of professional athletes have elevated CK-MM and CK-MB levels (Jaffe. 1984), Vassilis Mougios' 2007 paper "Reference intervals for serum creatine kinase in athletes" was the first to present a set of scientifically verified reference intervals for creatine kinase levels in athletes (Mougios. 2007).
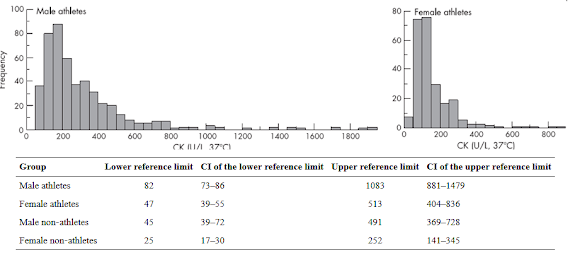 |
| Figure 2: Experimentally verified CK values in male and female athletes and calculated CK reference ranges for athletes and non-athletes (Mougious. 2014)) |
What you (could) have learned today: Before we are about to take a closer look at the "liver values" ALT and AST, next week, let's briefly summarize what you you could have learned today that may help you, when you're summoned to the doctors office and your doctor wants to call the ambulance to save your kidneys from the consequences of your "rhabdo":
Reference:- Elevations of >10,000IU can occur and last for days after intense workouts.
- Regular training lowers the exercise induced CK leakage from the 10,000+ range back to the 500-1,500IU range.
- Nevertheless, the CK levels of athletes will always be higher than that of sedentary controls.
- It can take up to a week for your CK levels to return to baseline. If you want to make sure that your high CK levels are caused by exercise and nothing else, you will have to take a full week (best 14-days) off, before you retest.
- Jaffe AS, Garfinkel BT, Ritter CS, Sobel BE. Plasma MB creatine kinase after vigorous exercise in professional athletes. Am J Cardiol. 1984 Mar 1;53(6):856-8.
- Karras DJ, Kane DL. Serum markers in the emergency department diagnosis of acute myocardial infarction. Emerg Med Clin North Am. 2001 May;19(2):321-37. Review.
- Mougios V. Reference intervals for serum creatine kinase in athletes. Br J Sports Med. 2007 Oct;41(10):674-8. Epub 2007 May 25.