![]() |
| Unless you're planning to just sit, instead of cycle on your spinning bike, it is by no means sure if your performance well benefit or maybe even suffer from the use of AMPK mimetics and activators. |
Recently someone asked me on Facebook, whether AMPK activators like Lipoic acid (ALA), Berberine, Metformin, AICAR & Co wouldn't make excellent performance boosters. I pondered that question for some time and said: "If you are about to compete in a highly glycolytic sport, the opposite is probably the case."
There's little question that supplements like lipoic acid are useful if you are an overweight type II diabetic. But let's be honest: How many of you fall into this category? As healthy, active individuals or even athletes, on the other hand, you should be aware that the ability of these agents to increase the glucose uptake and block the glyconeogenic pathways in the liver may easily make you run out of fuel during anaerobic activities like lifting or sprinting.
Learn more about hormesis and how antioxidants can also impair your gains ![]()
Is Vitamin E Good for the Sedentary Slob, Only?
![]()
Even Ice-Baths Impair the Adapt. Process
![]()
Vit C+E Impair Muscle Gains in Older Men
![]()
C+E Useless or Detrimental for Healthy People
![]()
Vitamin C and Glucose Management?
![]()
Antiox. & Health Benefits Don't Correlate
This does not negate the fact that AMPK activators, by their ability to increase the use of free fatty acids as a substrate,
may be of interest to endurance runners or athletes competing in other sports, where the lion's share of the energy they use during their workouts and competitions are carboxylic acids with a long aliphatic tail (chain), i.e. fatty acids.
Against that backround it is hardly surprising that the few pertinent studies that exist are - at least in parts - contradictory. Shortly before the last Olympic Games in Beijing, for example, a study was published that showed that the research chemical and AMPK activator AICAR (5-amino-1-b-D-ribofuranosyl-imidazole-4-carboxamide) increased the running capacity of mice
without any training. But let's be honest: Do you think athletes would be looking for agents that work without training... well, obviously they would, but AICAR - as potent as it may be - will never replace the blood, sweat and tears athletes have to invest to be successful. That's for sure.
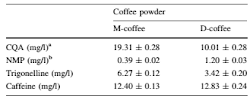
Which AMPK activators are actually prohibited by the WADA? The WADA list of prohibited substances lists only "AMP-activated protein kinase (AMPK), e.g. AICAR; and Peroxisome Proliferator Activated Receptor δ (PPARδ) agonists e.g. GW 1516" which is pretty unspecific and leaves me questioning whether other natural AMPK activators like ALA, berberine, chlorogenic acid or the most widely used one, i.e. metformin, would be illegal, too.
Nevertheless, the observation Narkar et al. (2008) made was enough for the World Anti-Doping Agency (WADA) to include certain AMPK activators in the list of forbidden drugs - for all, not just endurance sports, obviously.
![]() |
| Table 1: Adenosine monophosphate-activated kinase activators and their impact on exercise capacity (Niederberger. 2015) |
Actual experimental evidence of performance enhancing effects exists for several natural and synthetic AMPK mimetics and activators (see
Table 1). If you look closely, however, you will notice that all those "enhacnements" and "increases" have been in rodent models and/or non-athletes.
What does the latest review say? As usual, the special needs of Olympic-lifters, bodybuilders, sprinters and all other athletes who are competing in anaerobic sports are ignored by the authors of the latest and - as far as I know - first review of the impact of the activation of AMPK on sports performance.
![]() |
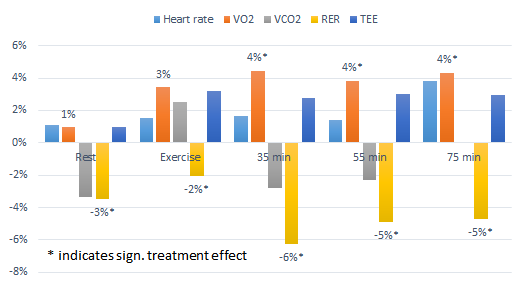
| It's the increase in the total time and endurance as well as VO2 in a injection only (no training) rodent study observed by Narkar et al. in 2008 that is behind all the hype around AICAR as a "potent doping agent". I wonder if the athlete who use is even know that the mice in the study didn't even train. Whether the effect is additive is thus highly questionable. |
In spite of their unfortunate ignorance of sports-specific differences, Niederberger et al. (2015) produce a neat overview of the available research on AMP mimetics like AICAR, pharmacological drugs like metformin, salycilic acid, thiazolidinediones, Phenobarbital and Telmisartan, and natural AMPK activators like green tea, capsaicin, resvertrol and co. Of these, none has been tested in athletes, though, even the applauded AICAR helps only
in theory (!). Unlike Niederberger's review suggests, the performance enhancing effects in studies like (Hayashi. 1998; Cuthbertson. 2007; Narkar. 2008) were after all observed
in the absence of baseline training and are thus
not representative of what would happen in athletes who won't be dumb enough to believe that they don't even have to train if they are abusing AICAR.
The lack of relevant evidence for performance benefits in athletes that would be induced by AMPK mimetics, as well as the existing evidence that AMPK promoters like resveratrol, which don't target AMPK primarily, but must be thought of as potent antioxidants instead, entail the risk of
anti-hormetic effects (e.g. the attenuation of the positive effects of endurance exercise on inflammatory and oxidative stress markers in aged men in response to 250mg resveratrol day in Olesen et al.'s 2014 study) put a huge "?" behind the actual usefulness of AMPK mimetics and promoters as athletic performance enhancers..
In the absence of experimental evidence from both rodent and human studies that involve AMPK activators and
anaerobic exercise, we have to use our brains to find out whether sprinters, bodybuilders, or weight lifters and athletes competing in team sports that have both an aerobic and an anaerobic component would benefit as well. In this case the extensive research on alpha lipoic acid (ALA) can help us, but we should not forget that the effects may differ from one agent to the other.
Due to the previously mentioned potentially negative effect on blood glucose in insulin sensitive individuals that is mediated primarily by increases in whole body glucose oxidation, increased glycolysis (wasting of the glycogen reserves| Barnes. 2004) and a reduced ability to produce new glucose "on demand" (via gluconeogenesis, which is AMPKs main of glucose control according to Zhang et al. 2009), athletes competing in anaerobic sports may in fact run the risk of running low on blood sugar and thus compromising their performance and/or being even more reliant on sugary high carbohydrate beverage.
![]() |
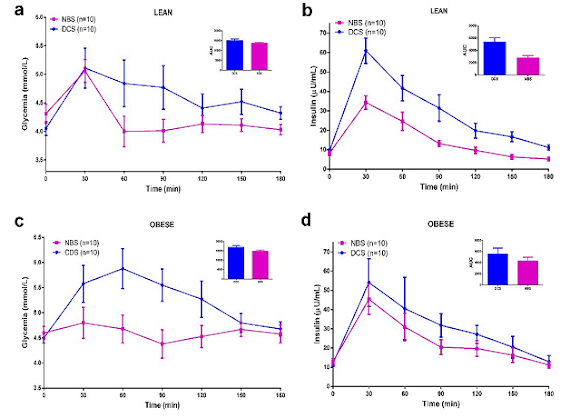
| In insulin sensitive muscle cells ALA reduces the rate of glycogen synthesis (Dicter. 2002). This should remind you of this simple truth: What's good for your obese neighbor, ain't necessarily good for you. Plus: ALA ain't the only supplement with different, often opposite effects in lean vs. obese. |
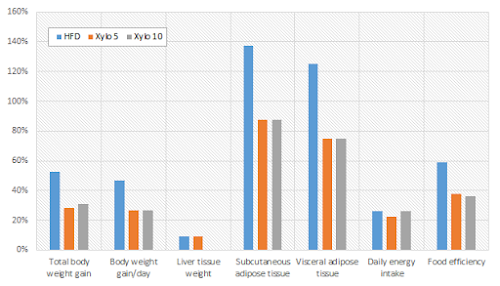
What's good for the obese is rarely good for athletes: The reduced protein synthesis (Figure 1) is only one of several undesirable side effects of high doses of ALA. One that people usually won't even believe exists is an impairment of glycogen synthesis in insulin sensitive skeletal muscle. While ALA is famous for partly restoring the whole body (including body fat) glucose uptake in insulin
resistant individuals, studies like the one by Dicter et al. (2002) indicate that it will
reduce the insulin-induced glycogen synthesis if the muscle in question is not insulin resistant, but
sensitive. That's an effect that may occur only at higher dosages of ALA (and other potent AMPK activators), but still one that no athlete can ignore.
If you don't care about blood glucose, you may be intrigued to hear that AMPK will not act on your glucose metabolism, alone. Increasing levels of AMPK will also
suppress skeletal muscle protein synthesis (
Figure 1), which is a side effect that's probably even worse than the remote risk of hypoglycemia, specifically in athletes competing in anaerobic sports.
![]() |
| Figure 1: Changes in p-AMPK and nutrient-induced protein synthesis in myotubes from the EDL muscle (Saha. 2010). |
Now, some of you may argue that I personally wrote in an
older article in the
Intermittent Fasting Series that the rise in AMPK due to exercise would not be a problem.
If you'd read
that article carefully, though, you'd also know that this is because exercise triggers the release of a
specific form of AMPK that's different from the one that's released during fasting and in response to regular AMPK activators. It is thus not unlikely that high(er) intakes of ALA as they would probably be abused by athletes, who (falsely) believe they'd benefit from it, can impair the protein synthesis to a similar extent as it was observed by Saha et al. in their 2010 study in rodent EDL muscles.
Furthermore animal studies show that chronic administration of albeit very high doses of ALA, equivalent to ~5g/day for a human being, will actually trigger significant reductions in lean mass (Shen. 2005) - something almost every athlete who's competing in anaerobic sports will want to avoid.
The answer to the question in the headline is - as so often: "It depends!" If you are an endurance athlete, the
acute, yet not the chronic consumption of the AMPK mimetics (=acts just like) like AICAR and maybe some of the less potent AMPK activators could improve your endurance. Without studies where the rodents (or even better men and women) are actually trained, even this assumption is speculative.
![]() |
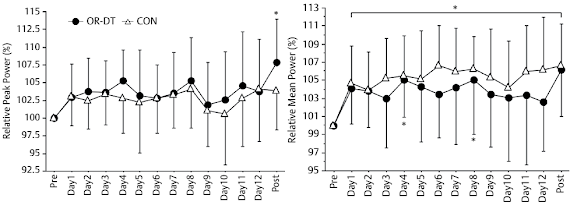
| Figure 2: While the last word has not been spoken, yet the impaired adaptive response to stressors in older subjects supplementing w/ 250mg/day resveratrol Olsen et al. observed in 2014 is further evidence that the chronic consumption of potent antioxidants (which happen to be AMPK promoters in this and other cases like ALA) must not be recommended unconditionally for athletes based on the available evidence. |
If, on the other hand, you're competing in sports where anaerobic performance, i.e. power, speed and other parameters that will critically depend on the availability of glucose, you will probably see no beneficial and, in the worst case, detrimental effects.
These detrimental effects could also occur in response to the chronic ingestion of AMPK promoters like
lipoic acid due to their potentially negative effect on protein synthesis and glycogen repletion, as well as in response to the chronic use of potent anti-oxidants for which
evidence exists that they impair the hormetic response to exercise and may thus be detrimental for athletes competing in both anaerobic and aerobic sports.
If you take small amounts of berberine, ALA, resveratrol, or other agents that have been shown to exert their health benefits via AMPK, though, it is
very unlikely that the previously discussed unwanted side effects surface (don't expect direct ergogenic effects, though). Moderation is - as so often - the key to perfect happiness |
Comment on FB!
References:
- Barnes, Brian R., et al. "The 5′-AMP-activated protein kinase γ3 isoform has a key role in carbohydrate and lipid metabolism in glycolytic skeletal muscle." Journal of Biological Chemistry 279.37 (2004): 38441-38447.
- Cuthbertson, Daniel J., et al. "5-Aminoimidazole-4-carboxamide 1-β-D-ribofuranoside acutely stimulates skeletal muscle 2-deoxyglucose uptake in healthy men." Diabetes 56.8 (2007): 2078-2084.
- Hayashi, Tatsuya, et al. "Evidence for 5′ AMP-activated protein kinase mediation of the effect of muscle contraction on glucose transport." Diabetes 47.8 (1998): 1369-1373.
- Narkar, Vihang A., et al. "AMPK and PPARδ agonists are exercise mimetics." Cell 134.3 (2008): 405-415.
- Niederberger, Ellen, et al. "Activation of AMPK and its Impact on Exercise Capacity." Sports Medicine (2015): 1-13.
- Olesen, Jesper, et al. "Exercise training, but not resveratrol, improves metabolic and inflammatory status in skeletal muscle of aged men." The Journal of physiology 592.8 (2014): 1873-1886.
- Saha, Asish K., et al. "Downregulation of AMPK accompanies leucine-and glucose-induced increases in protein synthesis and insulin resistance in rat skeletal muscle." Diabetes 59.10 (2010): 2426-2434.
- Shen, Q. W., et al. "Effect of dietary α-lipoic acid on growth, body composition, muscle pH, and AMP-activated protein kinase phosphorylation in mice." Journal of animal science 83.11 (2005): 2611-2617.
- Zhang, Bei B., Gaochao Zhou, and Cai Li. "AMPK: an emerging drug target for diabetes and the metabolic syndrome." Cell metabolism 9.5 (2009): 407-416.