|
| LLLT has also been shown to improve the appearance of cellulite (Jackson. 2013) | Learn more about what really helps against cellulite in this SV Classic |
Learn more about the nuances of dieting and fat loss here, at the SuppVersity
![]()
Orgasm Hormone Increases REE![]()
9 Tricks to Keep You REE Up![]()
High EAA Intake, High REE![]()
You're not a Bomb Calorimeter![]()
Calorie Shifting for Max. Fat Loss![]()
Met. Damage in Big Losers?
But let's return to the study at hand: Manageable and useful, in this case, meant three exercise sessions per week with 30 minutes of aerobic training and 30 minutes of resistance training per session.
Orgasm Hormone Increases REE

9 Tricks to Keep You REE Up

High EAA Intake, High REE

You're not a Bomb Calorimeter

Calorie Shifting for Max. Fat Loss

Met. Damage in Big Losers?
"During the intervention period, the voluntaries [sic!] followed a combined exercise training therapy. The protocol was performed three times per week and included 30 minutes of aerobic training and 30 minutes of resistance training per session. The aerobic training consisted of running on a motor-driven treadmill (Movement®) between 70 and 85% of maximal heart frequency, which was determined previously by treadmill submaximal test. The resistance exercise training was composed using exercises for the main muscular groups: bench press, leg press, sit-ups, lat pull-down, hamstring curls, calf raises, Straight-Bar Cable Curl (biceps), triceps pushdown, adductor and abductor chairs [see Table 1]. Training loads were successively adjusted, with volume and intensity being inversely modified and the number of repetitions being decreased to between 6 and 20 repetitions for three sets. The training loads were adjusted in each training session and evaluated according to the increase in participants’ strength. Thus, the training was conducted with maximal repetitions (RM)" (Sene-Fiorese. 2015).For the study, the scientists recruited a total of 64 adult obese women via classic newspapers and magazines as well as electronic media, TV and radio. The inclusion criteria were (i) primary obesity, body mass index (BMI) between 30 and 40 kg/m², (ii) age between 20 and 40 years old. Exclusion criteria were (i) the use of cortisone, anti-epileptic drugs; (ii) history of renal disease; (iii) alcohol intake; (iv) smoking; and (v) secondary obesity due to endocrine disorders. The inclusion and exclusion criteria were assessed by clinical evaluation by physician (endocrinologist).
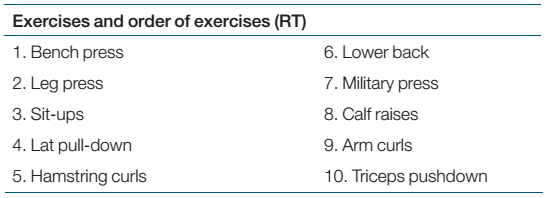 |
| Table 1: The scientists a resistance training protocol that had previously been used in Foschini (2010) |
This is a placebo controlled study! I think it's worth highlighting the fact that both groups believed they'd received the treatment, because all subjects had to go to the phototherapy sessions, but the device was actually turned on only for those in the ET-PHOTO, not for those in the ET-SHAM group.
In the ET-SHAM group the device which emits light at a wavelength that's too long for the human eye to actually see it was turned off. Thus the subjects in the SHAM = control group received a simulated phototherapy application ... and yes, that's basically the same thing as the "placebo group" in your average supplement study..  |
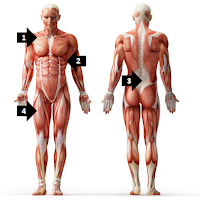
| Figure 1: Photo of the Device, Illustration of the Area of Application; Device Information, Irradiation and Treatment Parameters (Sene-Fiorese. 2015). |
"The phototherapy equipment was developed by Laboratory Technology Support-LAT, Center for Research in Optics and Photonics Institute of Physics in São Carlos city at University of São Paulo-USP. The device is a prototype equipment that was submitted for registration as a new patent. The device is composed of four plates made of rubberized material measuring 20 by 20 centimeters (cm) each. Each two plates are connected to an electronic control box. The emitters of Ga-Al-As diode Lasers are distributed in the plate every 2.5 cm, totaling 16 emitters per plate and 64 emitters in total. The prototype is illustrated and irradiation parameters are [mentioned in Figure 1]" (Sene-Fiorese. 2015).As I already hinted at in the previous paragraph, 805 nm is a pretty high wavelength. It's classified as near-infrared (near as in "near, but not in the visible spectrum"), which is too "long" to be seen by human beings... what it was not too long for, though, was to augment the beneficial effects the 48 workouts the subjects performed over the whole study period had on the women's body composition and metabolic health.
 |
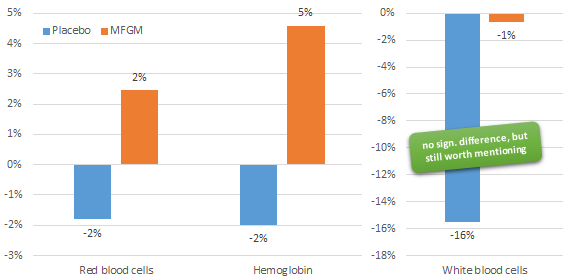
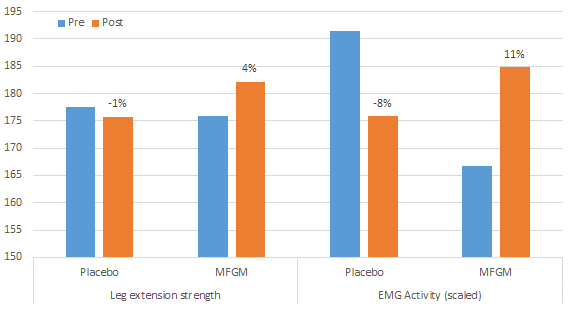
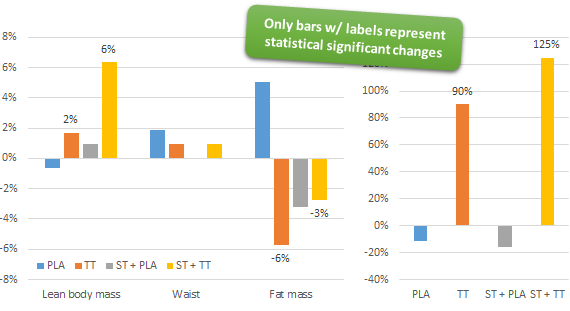
| Figure 1: Overview of the changes in body comp and glucose metabolism in both groups (Sene-Fiorese. 2015). |
If we also take into account that the the scientists observed similarly profound differences when they analyzed the subjects adiponectin levels, which decreased by 7% in the SHAM group (bad) and increased by a whopping 20% (good!) in the PHOTO group, it's really hard to argue that the benefits wouldn't be worth the hassle, even though one may question the accuracy of the body fat / lean mass data which was measured with a body impedance, instead of a DEXA device. Since the overall results do support significant additive effects, there's simply no reason to assume that the BIA data would be incorrect. In addition, BIA is actually relatively useful if you measure relative changes in body composition. If you want a correct one-time reading of your body fat, though, I wouldn't rely blindly on what a BIA device says.
Bottom line: As the authors point out, their latest study "demonstrated for the first time that phototherapy enhances the physical exercise effects in obese women undergoing weight loss treatment promoting significant changes in inflexibility metabolic profile" (Sene-Fiorese. 2015). While I would probably have replaced the grammatically questionable and nondescript phrase"inflexibility metabolic profile" with something more tangible like "insulin sensitivity" or "glucose control," Sene-Fiorese's conclusion is generally right.
Furthermore their findings may be somewhat surprising, but they are by no means unrealistic in view of the existing evidence that demonstrates that phototherapy (or low-level-laser-therapy | LLLT) is effective as an adjuvant tool in non-invasive body countering. It has been shown to help w/ the reduction of cellulite, fatigue, pain, blood circulation, wound healing, lipid metabolism and recovery after exercise (Neira. 2002; Ferraresi. 2010; Aquino. 2013; Paolillo. 2013; Houreld. 2014), as well as to increase the mitochondrial activity in irradiated cells by up-regulating genes involved in the mitochondrial complexes (Masha. 2013).
Unfortunately, our understanding of the underlying mechanisms that make LLLT so effective is still in its infancy. It is yet most likely that they are mediated on a cellular level by increases in PGC-alpha (the mitochondria builder) and sirtuins like SIRT-1. These proteins are all important regulators of mitochondrial function; and as you may remember from previous SuppVersity articles, they are also activated by resveratrol and a bunch of other supplements that have been shown to increase the health of the cells' mitochondria. How exactly the previously reported increases in muscle gains or the profoundly accelerated fat loss in the study at hand are brought about, will have to be elucidated in future studies, though | Comment on Facebook!
References: |
| The same LLLT therapy has also been shown to almost double the muscle gains in a study with an 8-week eccentric training program | more |
Unfortunately, our understanding of the underlying mechanisms that make LLLT so effective is still in its infancy. It is yet most likely that they are mediated on a cellular level by increases in PGC-alpha (the mitochondria builder) and sirtuins like SIRT-1. These proteins are all important regulators of mitochondrial function; and as you may remember from previous SuppVersity articles, they are also activated by resveratrol and a bunch of other supplements that have been shown to increase the health of the cells' mitochondria. How exactly the previously reported increases in muscle gains or the profoundly accelerated fat loss in the study at hand are brought about, will have to be elucidated in future studies, though | Comment on Facebook!
- Aquino Jr, Antonio E., et al. "Low-level laser therapy (LLLT) combined with swimming training improved the lipid profile in rats fed with high-fat diet." Lasers in medical science 28.5 (2013): 1271-1280.
- Ferraresi, Cleber, et al. "Effects of low level laser therapy (808 nm) on physical strength training in humans." Lasers in medical science 26.3 (2011): 349-358.
- Foschini, Denis, et al. "Treatment of obese adolescents: the influence of periodization models and ACE genotype." Obesity 18.4 (2010): 766-772.
- Houreld, Nicolette N. "Shedding light on a new treatment for diabetic wound healing: a review on phototherapy." The Scientific World Journal 2014 (2014).
- Masha, Roland T., Nicolette N. Houreld, and Heidi Abrahamse. "Low-intensity laser irradiation at 660 nm stimulates transcription of genes involved in the electron transport chain." Photomedicine and laser surgery 31.2 (2013): 47-53.
- Neira, Rodrigo, et al. "Fat liquefaction: effect of low-level laser energy on adipose tissue." Plastic and reconstructive surgery 110.3 (2002): 912-922.
- Paolillo, Fernanda Rossi, et al. "Infrared LED irradiation applied during high-intensity treadmill training improves maximal exercise tolerance in postmenopausal women: a 6-month longitudinal study." Lasers in medical science 28.2 (2013): 415-422.
- Sene‐Fiorese, Marcela, et al. "The potential of phototherapy to reduce body fat, insulin resistance and “metabolic inflexibility” related to obesity in women undergoing weight loss treatment." Lasers in Surgery and Medicine (2015).