 |
| In today's installment: Alpha-GCP and reduces thyroid function; accurate body fat measurement in contest prep confirms recomp effect; more protein keeps shift workers lean and healthy. |
Fasting and alpha-GPC have sth in common: Nootropic, pro-GH (initially), anti-thyroid effects

Breakfast and Circadian Rhythm

"Lean Gains" Fast Works

Habits Determine Effects of Fasting

Fasting Works for Obese, Too!?

IF + Resistance Training = WIN

ADF Beats Ca-lorie Restriction
- Alpha-GCP, nootropic and alleged GH booster, impairs thyroid function? To answer this question in the affirmative, the data Bellar et al. presented at #ISSN17 is clearly not sufficient. It is, however, interesting to note that Bellar's experiment in forty-eight healthy clearly confirmed the authors' hypothesis that "increasing CNS acetylcholine can affect dopamine levels, which can, in turn, affect other hormones such as Thyroid stimulating hormone (TSH)" (Bellar 2017).
![]()
To test this hypothesis, the researchers from the University of Louisiana at Lafayette, the Louisiana State University, and Ball State University fed the aforementioned young men 500 mg A-GPC, 250 mg A-GPC, or Placebo. Within 1-2 h after the ingestion of the supplement, the authors found that...- serum free choline was significantly elevated in the two A-GPC groups as compared to placebo (132% and 59% respectively)
- serum TSH was significantly depressed in the 500 mg A-GPC group compared to other treatments (p < 0.04).
What's the verdict on alpha-GPC and your thyroid?
It's as simple as "big effect = big side effect". You cannot have the soothing effect of increased CNS acetylcholine without its "downsides". Without knowing how long/if the effects on TSH and thus downstream effects on the production of thyroid hormones persist, there's no reason to panic, though.
Moreover, if alpha-GPC does what it's advertised for, the TSH suppression could also be a result of a growth hormone surge (Kawamura 2012). GH depresses the secretion of thyrotropin and thus TSH, but by increasing the peripheral conversion of thyroxine to triiodothyronine, the occasional transient GH spike from alpha-GPC will not have your metabolism tank... let alone trigger hypothyroidism. What would happen in response to chronic administration of alpha-GPC is still up in the open, though.![]()
Figure 1: The reduction in TSH could be a response to the increase in GH many supplement users are actually aiming to achieve when they consume alpha-GPC supplements. If that's the case, the decreased TSH can be expected to be as transient as the increase in growth hormone (which is btw. irrelevant for your gainz, bro).


Warning - the studies discussed in this series are not yet peer-reviewed and published! Since the write-up is based on abstracts, only. I cannot discuss and scrutinize the results with the same degree of detail and healthy skepticism you're used to from other SuppVersity articles.
- You cannot shed body fat and gain muscle at the same time? Yes, you can! One of the reasons people tend to blow up to crazy body fat levels when bulking is the still prevalent believe that you'd have to be in a significant caloric surplus to pack on muscle. In fact, I overheard a trainer at the gym tell a skinny fat rookie only recently: "You got to eat... you need a big energy to gain muscle."
![]()
Many active and retired practitioners, on the other hand, often talk about "recomp" and thus refer to losing fat and adding muscle to their frames simultaneously. One of the poster presentations at #ISSN17 seems to suggest that - at least in the early phase of a drug-free contest prep - this is exactly what's happening.
Using a former NCAA Division II athlete who had previously competed in 4 physique competitions, Grant M. Tinsley tried to elucidate more information about the way(s) the human body changes when it is exposed to a carefully timed and balanced combination of diet and exercise intended to maximize fat and minimize muscle loss. At the commencement of the study, the subject was beginning an 18-week preparation phase prior to competing in a National Physique Committee (NPC) competition in the Figure division. Tinsley further explains:![]()
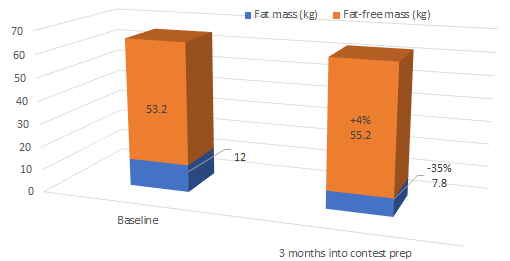
Figure 2: The case study shows: When you combine exercise and diet in the right way(s) you can gain lean mass (+4%) and lose body fat (-35%) - data measured using the 4-C model (Tinsley 2017). "Throughout the preparation phase, the athlete was closely advised by her coach, a competitive bodybuilder with 20+ years of coaching experience. The athlete meticulously tracked dietary intake, supplement use and exercise sessions. Additionally, the athlete was assessed monthly in the university research laboratories" (Tinsley 2017).
These assessments included dual-energy x-ray absorptiometry (DXA) and multi-frequency bioelectrical impedance analysis (MF-BIA). Body volume and total body protein were calculated using DXA output (Wilson 2013, body composition was assessed using the 4-compartment model as described by Lohman & Going (Lohmann 1993).

 |
| Figure 3: The use of a 4-compartment model to assess body composition is a strength of this case study at hand because it isn't as easily fooled as the DXA alone as it was used in Wilson's recent keto paper I wrote about recently (illustration from Ellis 2000) |
More from another ISSN#17 paper: If you're not working with athletes, but overweight/obese clients, your best choice, next to the 4c model, is air displacement plethysmograph (ADP | BodPod). Of the latterTrexler et al. (2017) reported at #ISSN17 that it "provided more valid estimates for cross-sectional and longitudinal changes in body composition in comparison to DXA and US" (Trexler 2017) - with DXA performing better than ultrasound.
- Based on 4-compartment calculations, Tinsley reports that "the athlete’s body fat decreased from 18.3% to 12.3% over the first 3 months of preparation" (Tinsley 2017). This alone wouldn't be surprising. The fact that, Tinsley observed concomitant decreases in fat mass (12.0 kg to 7.8 kg) and increases in fat-free mass (53.3 kg to 55.2 kg), on the other hand, is noteworthy.
What's the verdict on 'recomp'?
In view of the existence of several RCTs that showed concomitant increases in muscle mass and decreases in fat mass in obese individuals who were subjected to combined diet and (resistance) training, the 'news' here is that this works with lean(er, more) athletic people as well. With that being said, Trexel et al. reported very similar results from a mixed cohort of fifteen physique athletes - 7 male, 8 female drugfree (according to interviews) athletes competing in bikini (n=7), figure (n=1), physique (n=5), or bodybuilding (n=2) classes. In case you missed this one, you can read up on it here!
What? You're asking yourself why the Tinsley study still made the cut, if Trexel's study had more subjects, featured both, men and women, and was already discussed at length? Well, Tinsley used the "gold-standard 4-compartment model", Trexel et al. "only" amplitude-mode ultrasonography and skinfold measurements. Just like classic DXA scans of which Tinsley observed that "it substantially overestimated body fat percentage in the observed athlete" these methods have a comparatively (vs. 4-C) high margin of error (see info box). To point you to a study using the 4-C model was thus (IMHO) useful.
- Health care workers' protein intake may determine their body composition and health. More protein = leaner and healthier? Likewise right from #ISSN17 is the insight that "surpassing general PRO recommendations (0.8 g/kg) may advantageously influence body composition and blood lipid profile" (Pihoker 2017) - highly advantageous in terms of body weight, BMI, body fat, and blood lipids (see Figure 4).
![]()
Before you rejoice, however, please note: This insight was phrased based on observational data from thirty-three female healthcare shift-workers (Mean ± SD: age = 30.6 ± 9.2 yrs, height = 164.7 ± 6.8 cm, weight = 66.5 ± 10.2 kg, body mass index (BMI) = 24.5 ± 3.7 kg/m2) who were tested following a minimum eight-hour fast. That's not 'bad', but it's not the result of a randomized controlled study, which leaves room for a lot of uncontrollable confoundable variables such as 'people who eat more protein are generally more health-conscious, work out more regularly and/or consume overall healthier diets'.
At least one of these potential confounders could be excluded by the scientists, though. Next to being scanned with DXA to assess fat mass (FM), lean mass (LM), bone mineral content (BMC), and body fat percentage (%fat), the subjects also filled three-day dietary logs (2 workdays, 1 off-day) based on which the scientists estimated the average kilocalorie (kcal), carbohydrate (CHO), PRO, and fat intake. For the final analysis, participants were initially stratified into two groups using protein intake of ≥ 1.2 g/kg bodyweight (‘adequate’, n=15) or <1.2 g/kg BW (‘deficient’, n=18). Between-group differences were evaluated using a series of independent t-tests. Relationships between dietary intake estimations (kcal, PRO, CHO, and fat) and body composition and blood variables were analyzed using Pearson’s bivariate correlations.
The results of this battery of tests revealed that the subjects in the "adequate protein" group (the scientists words), i.e. those who consumed more than 150% of the RDA per day had -10.81±2.89 kg (p=0.001) lower body weights, significantly less body fat (∆=6.73±2.34 kg, p=0.008), lower levels of pro-atherogenic non-HDL cholesterol (∆=17.09 ± 7.83, p=0.037), and a comparatively low ratio of total to HDL cholesterol (TC:HDL ∆=0.54±0.25, p=0.039) that's indicative of a significantly reduced risk of heart disease.
In that, it is interesting to note that no other dietary variable correlated significantly with these measures - neither the total energy intake, nor the "macros", i.e. the distribution of energy on proteins, fats and carbs [note: this does also mean, that there was no further benefit of even more protein].![]()
Figure 4: Body composition of shift workers w/ protein intakes >1.2g/kg vs. intakes <1.2g/kg (RDA = 0.8g/kg).
What's the verdict on high(er) protein intakes for health workers?
Again, we're just talking about observational data, but the lack of significant relationships between other/all measured dietary variables, body composition, and blood measurements does indeed, as the scientists write, "suggests that protein plays a special role in terms of the body composition and blood lipids in shift-working personnel. And let's be honest: Why shouldn't a protein intake beyond the demarcation line of 0.8g per kg/d do just that!?
The evidence in favor of the beneficial effects of high(er than RDA) protein diets on appetite is quite conclusive. If we take into consideration that high protein foods often replace/reduce the consumption of classic low protein snacks, any deliberate or unconscious increase in protein intake will - at least hypothetically - address two of the main nutritional problems of health-care shift-workers (Lowden 2010).
Moreover, data from Ishizuka et al. 1983 even suggests that high protein meals consumed at night may have an indirect and for shift-workers very welcome effect on the circadian rhythm as they, but not regular or high fat/high carb meals trigger a profound release of cortisol independent of the time of the day. In contrast to low protein meals, shift workers' circadian clock will thus get the same cortisol-related feedback (Åkerstedt 1978) in response to a meal at night as they'd get during the day - certainly no disadvantage in view of the fact that the latest research indicates that the weight and metabolic problems of shift workers are at least aggravated if not triggered by circadian desynchronization (Broussard 2016), which can, in turn, be triggered and (partially) reversed by food timing (Vetter 2017).


 |
| High Protein Breakfast Lowers Weight (8%), Waistline (4%) + HbA1c (12%) in T2DM - Especially if the Protein is Whey | read the full article |
If you insist on freaking out, do so if this is the first time you realize that any side effect of dietary supplements is, when all is said and done, just a regular effect you didn't pay for and (often) didn't expect to see. In that, the rule of thumb is: potent intended effect = potential for potent side-effect.
On 'recomping': While Tinsley's case study did observe a significant body-recomposition effect, it is important to note that even the 4-C model the scientist used isn't 100% accurate and that a 1.9kg change of lean mass measured in a single subject ain't enough to "prove" the claim that you can build muscle and lose fat concomitantly. Nevertheless, in conjunction with the increase in total body protein content (from 10.4 kg to 10.9 kg), the case-study at hand still adds to the evidence that this kind of 'recomp' isn't impossible to achieve - and that not just for the obese (there are several studies showing that diet + exercise can trigger fat loss + muscle gain in the obese), but also for normal-weight/even lean individuals.
The observational data on high-protein diets for shift-workers may, when assessed in isolation, not be very convincing. In view of what you've learned about the general effect of high(er) protein intake on food intake, body composition, and health, it does yet confirm an evidence-based hypothesis many of you probably already had. Plus: the potentially corrective circadian effects of high(er) protein meals at night I discussed in the corresponding subsection of this article would only add to the general metabolic benefits of increased protein intakes | Comment on Facebook!
References:
- Åkerstedt. "Circadian rhythms in the secretion of cortisol, adrenaline and noradrenaline." European journal of clinical investigation 8.2 (1978): 57-58.
- Bellar, et al. "Evaluation of the effects of two doses of alpha glycerylphosphorylcholine on thyroid stimulating hormone levels." Proceedings of the Fourteenth International Society of Sports Nutrition (ISSN) Conference and Expo (2017).
- Broussard, Josiane L., and Eve Van Cauter. "Disturbances of sleep and circadian rhythms: novel risk factors for obesity." Current Opinion in Endocrinology, Diabetes and Obesity 23.5 (2016): 353-359.
- Ellis, Kenneth J. "Human body composition: in vivo methods." Physiological reviews 80.2 (2000): 649-680.
- Ishizuka, B., M. E. Quigley, and S. S. C. Yen. "Pituitary hormone release in response to food ingestion: evidence for neuroendocrine signals from gut to brain." The Journal of Clinical Endocrinology & Metabolism 57.6 (1983): 1111-1116.
- Kawamura, Takashi, et al. "Glycerophosphocholine enhances growth hormone secretion and fat oxidation in young adults." Nutrition 28.11 (2012): 1122-1126.
- Lohman, Timothy G., and Scott B. Going. "Multicomponent models in body composition research: opportunities and pitfalls." Human body composition. Springer US, 1993. 53-58.
- Lowden, Arne, et al. "Eating and shift work—effects on habits, metabolism, and performance." Scandinavian journal of work, environment & health (2010): 150-162.
- Pihoker, et al. "Characterization of body composition, blood lipids, and nutrition profile in female healthcare shift-workers when stratified by protein intake." Proceedings of the Fourteenth International Society of Sports Nutrition (ISSN) Conference and Expo (2017).
- Tinsley, Grant M. "Substantial body recomposition during contest preparation in an experienced female figure competitor: results of 4-compartment model and total body protein calculations." Proceedings of the Fourteenth International Society of Sports Nutrition (ISSN) Conference and Expo (2017).
- Trexel, et al. "Estimating body composition at baseline and tracking changes during weight loss: Validity of common methods in comparison to a criterion four-compartment model." Proceedings of the Fourteenth International Society of Sports Nutrition (ISSN) Conference and Expo (2017).
- Vetter, Celine, and Frank AJL Scheer. "Circadian Biology: Uncoupling Human Body Clocks by Food Timing." Current Biology 27.13 (2017): R656-R658.
- Wilson, Joseph P., et al. "Improved 4-compartment body-composition model for a clinically accessible measure of total body protein." The American journal of clinical nutrition 97.3 (2013): 497-504.