 |
| This is what Photoshop and creativity can tell us about aging men. |
Virile men live longer! Ca. 30% longer, to be precise.
If you take a look at the link between serum testosterone, free testosterone and DHT and the all-cause mortality risk of the 16,451 community-dwelling older men from Perth in Western Australia it should be obvious that the third quartile of all these serum values, is where you want your androgen levels to be, if you intend to live to see your 90th birthday.
 |
| Figure 1: Relative reduction in all-cause mortality with total and free testosterone levels, as well as dihydrotestosterone levels in quartile 2,3 & 4 vs. quartile 1 (Yeap. 2013) |
Symptoms of low testosterone:
And while your androgen levels shouldn't be significantly lower, you also don't want them in the fourth quartile, where the all-cause mortality risk begins to rise again. Unless you don't want to lose the ~30% all-cause mortality of being in the zone, you shouldn't let the rumors about a causal (not corollary) link between testosterone replacement therapy (TRT) and the incidence of prostate cancer upset you. Why, well because ...Somatic: Gynecomastia, de- creased body hair, hot flashes, decreased lean muscle mass, decreased strength, anemia, frailty, osteoporosis, easy fatigue, sleep disturbances, increased body fat or body mass index
Psychological: Depressed mood, irritability, emotional lability, impaired cognition and memory, decreased energy
Sexual: Diminished libido, erectile dysfunction, decreased nocturnal and morning erections, difficulty achieving orgasm, decreased performance (Traish. 2011)."[...] to date, no study or review has definitively shown that androgen replacement therapy is an independent risk factor for development of prostate cancer." (Fisher. 2012)The thing you should ask yourself is thus whether you really want to give up on this 30% reduction in all-cause mortality, or the decrease in fatal cardiovascular events, Ramasay et al. list next to the reduction in body fat mass, and insulin resistance among the proven benefits of TRT in their 2012 review of the literature.
It's your decision and therefore you should make sure that it's you and not your doctor who takes this decision. If you decide to help your low testosterone levels along, it's your doctors job to help and assist you by ordering and interpreting regular hormone and, as Fisher et al. suggest, PSA tests.
Informed decisions, require information, lab values, and reference ranges!
Speaking about "interpreting" hormone panels. One of the problems you'll be facing is that nobody can actually tell you what your normal testosterone level should look like. Of course, every med-school graduate will believe that he knew exactly what's good for you, but when it's all said eand done, scientists (and doctors) tend to be a bit too egalitarian, when it comes to "normal ranges". So egalitarian, in fact that they simply assume that a lightweight Chinese pencil pusher must have the same testosterone levels as a 6.6 ft tall, 300lbs heavy Caucasian strongman.
 |
| Table 1: Normal ranges for total T. |
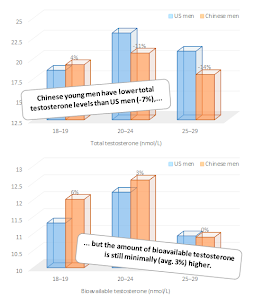 |
| Figure 2: Total and bioavailable testosterone levels in US and Chinese young men (Xu. 2013) |
By this means, the researchers wanted to find out whether the potentially existing differences in androgen levels in Caucasianvs. Asian young men would warrant a revision / specification of the "normal" range for men from different ethnic backgrounds.
As you can see the results are not exactly easy to interpret (Figure 2) - is this a difference, or not?
If we take another look at the data in Figure 2 and compare the relative differences between the total testosterone levels of young US vs. Chinese men to those that made a significant difference, in the previously discussed study by Yeap et al. (see Figure 1), we will have to concede that the xisting differences can hardly be significant. They are after all a magnitude smaller than the quartiles in the Yeap study.
Free vs. total testosterone, measured vs. calculated: Direct measurement of free testosterone levels is different from using the total testosterone and SHBG levels (which were higher in US men, by the way; Xu. 2013) to calculate an estimated amount of free testosterone (cf. Vermeulen. 1999). Since it's cheap and usually pretty accurate this is yet what most labs will do. You should however be aware that the values are accurate, only, if your SHBG and albumin values are "normal" as well. If those are out of range, it's a good idea to get the free testosterone levels measured directly, to find out where you are standing.
That being said, there are at least three additional reason that speak against establishing specific testosterone cut-off values for different ethnic groups based on the Xu study:- The Xu study is not representative of "all" Chinese young men: The Xu study compares US citizens in the US to Chinese citizens in China. Who tells us that the values they obtained for young Hong Kongers are valid for 2nd generation Chinese immigrants to the US, as well? Environmental conditions, dietary factors, etc. all that could just as well be the reason for the measured differences as ethnicity-specific genetic differences.
- The Xu study, or rather the NHANES data is not representative of a specific ethnicity: By analogy to (1), the Xu study, which uses data from NHANES III to gauge the average testosterone levels of male US citizens, relies on data from Asian, African American, Native American, Hispanic and Caucasian US citizens. How on earth would you establish ethnicity specific normal values based on that?
- Using the Yeap study as a reference to determine "optimal levels" is unwarranted: With old men as study participants, the significance of the optimal total testosterone levels from the Yeap study (12.56 –15.75 mmol/L ≡ 362- 454ng/dL) is about as questionable as the assumption that older men are actually supposed to have significantly lower testosterone levels.
If you do that, i.e. compare free instead of total testosterone levels, you will find that the purported ethnic differences disappear. And this is true not solely for the comparison of the data from Chinese and US men Xu et al. analyzed, but also for the existing differences between Mexican-American, non-Hispanic black and non-Hispanic white men in the NHANES study by Rohrmann et al. (2007). Specific reference ranges for Asian, Caucasian, African American, Hispanics, ... are thus probably unwarranted (not sure about Aliens, though ;-).
The age related decline in testosterone is rapid: Accoring to Morley, et al. the average rate of decrement in testosterone concen-tration for men aged 60+ is 110 ng/dL every decade. A "normal" Caucasian man, who would still have a testosterone level of 500ng/dl when he's sixty (Rohrmann. 2013) would thus end up at 280ng/dl, which is right in the "highest risk of all-cause mortality" quartile (Q1) of the Yep study.
Bottom line: Despite the fact that our insights into the non-existent, or at least insignificant ethnic differences in free and total testosterone levels confirm the validity of the currently propagated "normal" ranges for young men, we are still left with the implications of the Yeap study and the questionable usefulness of "age adjusted" testosterone levels.
If we take into account that the age-induced androgen decline correlates with the aforementioned increases in all cause and cardiovascular mortality (Yeap. 2013), as well as lower levels of handgrip, hip flexors, hip extensors and abductors strength (Perry III. 2000) and an increase risk of development metabolic syndrome (48% higher risk; cf. Rodriguez. 2007), it would certainly appear that any "age-adjustment" that's based on observations in the average aging male is bogus...but I guess that's a topic for another SuppVersity article ;-)
If we take into account that the age-induced androgen decline correlates with the aforementioned increases in all cause and cardiovascular mortality (Yeap. 2013), as well as lower levels of handgrip, hip flexors, hip extensors and abductors strength (Perry III. 2000) and an increase risk of development metabolic syndrome (48% higher risk; cf. Rodriguez. 2007), it would certainly appear that any "age-adjustment" that's based on observations in the average aging male is bogus...but I guess that's a topic for another SuppVersity article ;-)
- Ramasamy, R., Fisher, E. S., & Schlegel, P. N. (2012). Testosterone replacement and prostate cancer. Indian journal of urology: IJU: journal of the Urological Society of India, 28(2), 123.
- Yeap, B. B., Alfonso, H., Chubb, S. P., Handelsman, D. J., Hankey, G. J., Almeida, O. P., ... & Flicker, L. (2013). In Older Men an Optimal Plasma Testosterone Is Associated With Reduced All-Cause Mortality and Higher Dihydrotestosterone With Reduced Ischemic Heart Disease Mortality, While Estradiol Levels Do Not Predict Mortality.
- Perry III, H. M., Miller, D. K., Patrick, P., & Morley, J. E. (2000). Testosterone and leptin in older African-American men: relationship to age, strength, function, and season. Metabolism, 49(8), 1085-1091.
- Rodriguez, A., Muller, D. C., Metter, E. J., Maggio, M., Harman, S. M., Blackman, M. R., & Andres, R. (2007). Aging, androgens, and the metabolic syndrome in a longitudinal study of aging. Journal of Clinical Endocrinology & Metabolism, 92(9), 3568-3572.
- Rohrmann, S., Nelson, W. G., Rifai, N., Brown, T. R., Dobs, A., Kanarek, N., ... & Platz, E. A. (2007). Serum estrogen, but not testosterone, levels differ between black and white men in a nationally representative sample of Americans. Journal of Clinical Endocrinology & Metabolism, 92(7), 2519-2525.
- Traish, A. M., Miner, M. M., Morgentaler, A., & Zitzmann, M. (2011). Testosterone deficiency. The American journal of medicine, 124(7), 578-587.
- Vermeulen, A., Verdonck, L., & Kaufman, J. M. (1999). A critical evaluation of simple methods for the estimation of free testosterone in serum. Journal of Clinical Endocrinology & Metabolism, 84(10), 3666-3672.
- Xu, L., Au Yeung, S. L., Kavikondala, S., Leung, G. M., & Schooling, C. M. (2014). Testosterone concentrations in young healthy us versus Chinese men. American Journal of Human Biology, 26(1), 99-102.